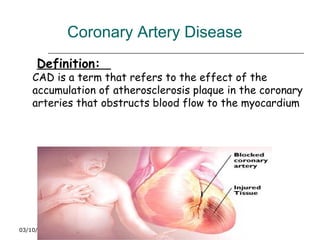
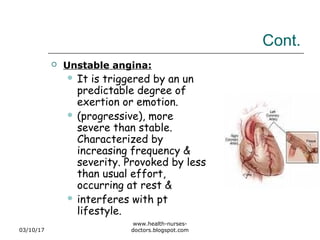
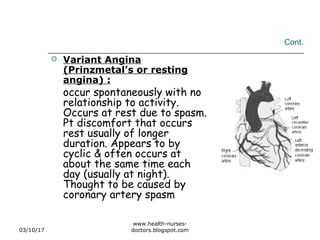
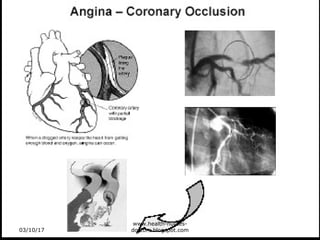
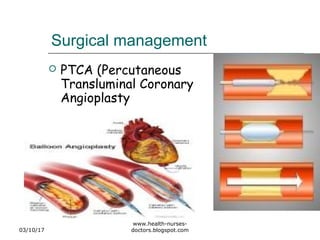
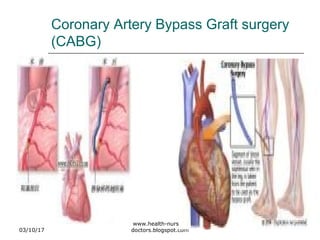
This document discusses coronary artery disease and two conditions that can result from it - angina pectoris and myocardial infarction. It defines angina pectoris as chest pain or discomfort due to reduced blood flow to the heart muscle, and describes the different types of angina including stable, unstable, and variant angina. Myocardial infarction is defined as the death of heart muscle tissue from a lack of oxygen supply. The document outlines the causes, symptoms, diagnostic tests, treatment options including medications, angioplasty and bypass surgery, nursing care, complications, prevention, and cardiac rehabilitation for these two coronary artery disease conditions.