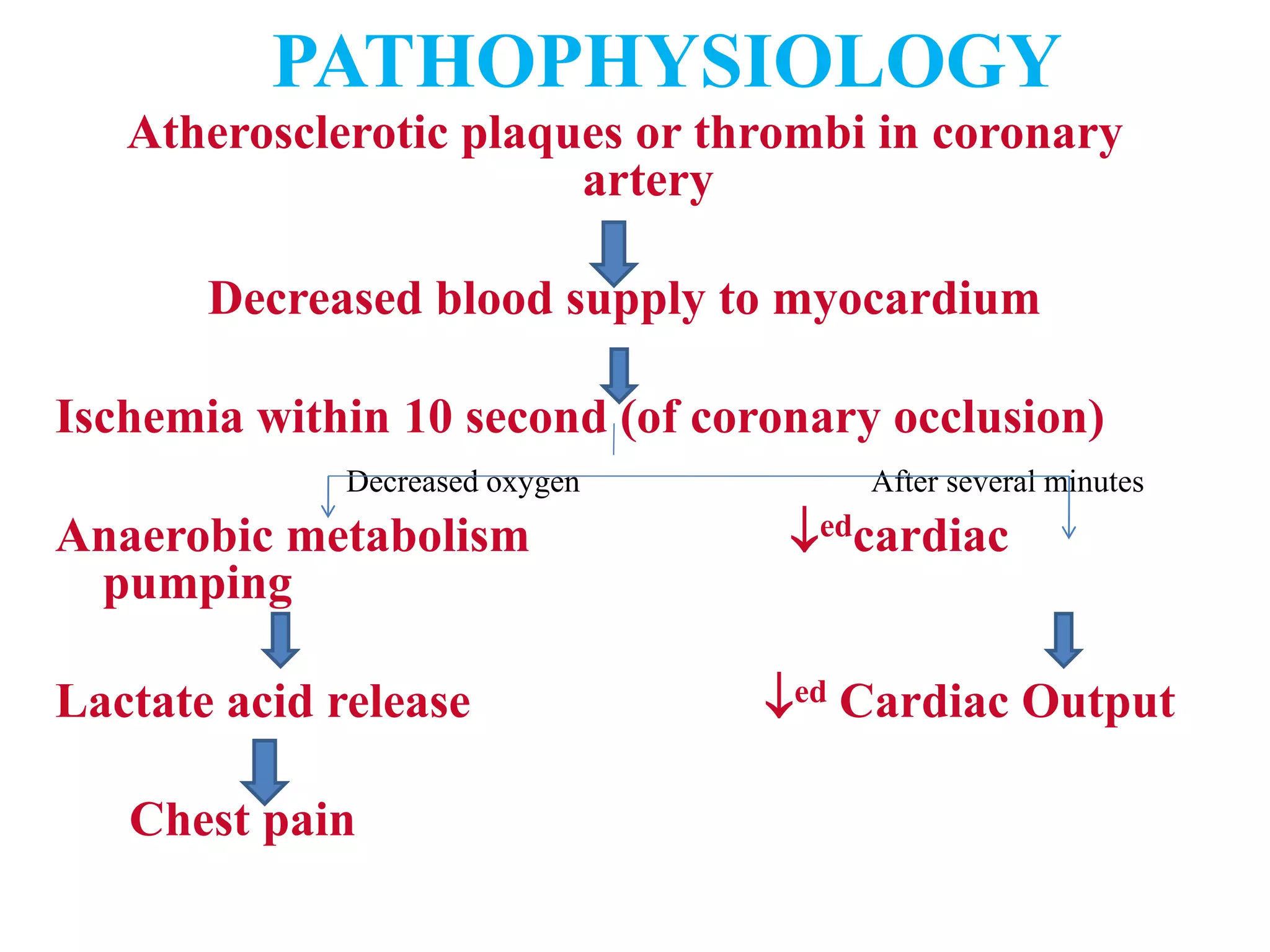
Coronary Artery Disease encompasses conditions involving obstructed blood flow through the coronary arteries, including acute myocardial infarction and angina pectoris. It is caused by atherosclerosis and the accumulation of fatty substances in arterial walls. Risk factors include age, family history, smoking, diabetes, hypertension, and high cholesterol. Symptoms vary depending on the location of blockages but may include chest pain and shortness of breath. Diagnosis involves ECG, cardiac enzymes, and angiography. Treatment focuses on lifestyle changes, medications, angioplasty, stents, or bypass surgery to improve blood flow.