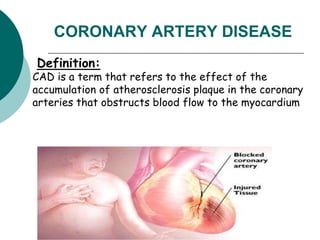
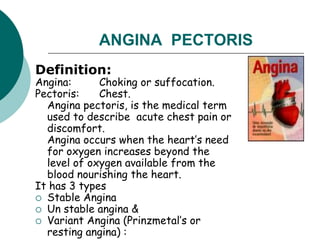
The document provides an overview of unstable angina and its relationship to coronary artery disease (CAD), explaining the definition, types, mechanisms, and clinical manifestations of angina. It details the complications of CAD, such as myocardial infarction, and outlines the importance of assessment and management strategies, including medication and lifestyle modifications. The document also highlights the significance of cardiac rehabilitation and patient education in recovery from myocardial infarction.





































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)

