•Sustained release isa drug delivery
method designed to release a
medication slowly over an extended
period of time.
•This is in contrast to immediate-release
medications, which are absorbed
quickly into the bloodstream.
What is Sustained Release?
3.
• A controlledrelease drug delivery system is a
formulation that releases medication at a
predetermined rate over an extended period.
• This technology maintains consistent drug levels in
the body, reducing dosing frequency and improving
treatment effectiveness.
• By controlling the release of medication, it
minimizes side effects and enhances patient
compliance.
What is Controlled Release?
4.
• Controlled drugdelivery systems can help retain drug levels
within a certain range, reduce the dosing frequency, maximize
the effectiveness of the medicine, and improve patient
compliance [1].
• The most essential and frequent justification for their appeal
is the ease to be administered. Carry-ability and
manufacturing on a large scale are both straightforward.
• Two criteria would be necessary if one needs to envision the
optimum drug delivery system. Initially, the dose for the
entire course of treatment should be solitary and especially
for the chronic ailments, as in the case of hypertension or
diabetes.
• Secondly, the delivery of active ingredient should be site
specific, thereby eliminating the toxicity for other
organs/tissues
Controlled Release…
5.
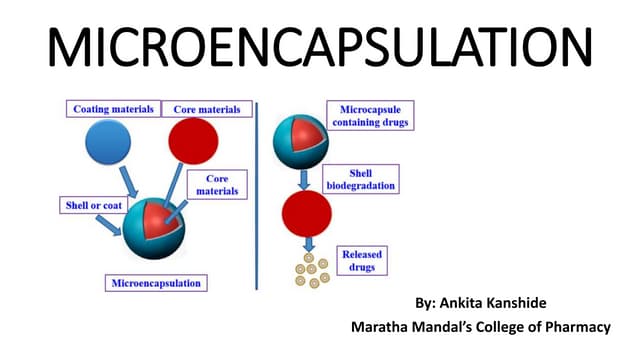
• The drugis encapsulated in a special formulation.
• This formulation allows for a gradual release of
the medication into the body.
How it works
6.
• The drugis encapsulated in a
special formulation.
• This formulation allows for a
gradual release of the medication
into the body.
Conventional Drug Delivery Systems
7.
• Administration: Thedrug is typically
administered orally in the form of tablets,
capsules, or liquids.
• Disintegration: Once the drug reaches the
stomach, it disintegrates or dissolves,
releasing the active ingredient.
• Absorption: The released drug molecules are
absorbed through the lining of the stomach
or small intestine into the bloodstream.
• Distribution: The drug is then transported
through the bloodstream to the target site
within the body.
• Therapeutic Effect: The drug exerts its
intended effect at the target site, addressing
the specific medical condition.
Immediate Release
8.
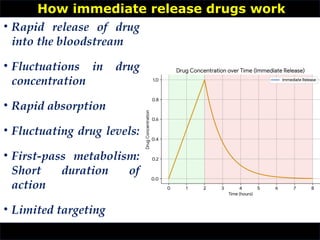
• Rapid releaseof drug
into the bloodstream
• Fluctuations in drug
concentration
• Rapid absorption
• Fluctuating drug levels:
• First-pass metabolism:
Short duration of
action
• Limited targeting
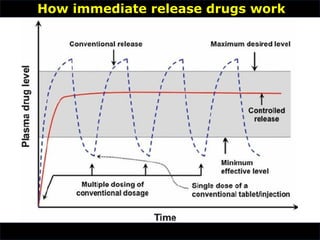
How immediate release drugs work
• Controlled release:
•Delivers drug at a constant
rate over time.
• Targeted delivery:
• Focuses on delivering drug
to specific site of action.
• Goal:
• Maintain constant
therapeutic drug level in
plasma.
• Mechanism:
• Balance between drug input
and elimination.
• Drug input:
• controlled release
formulation
• Drug output:
• metabolism, excretion (e.g.,
urine, feces)Mathematical
model: Rate in = Rate out
(kel * Cd * Vd)
Concepts
11.
•
Controlled vs. ConventionalRelease
Controlled release: Conventional release:
• Maintains consistent drug
levels (therapeutic range)
• Fluctuating drug levels
• Improves patient compliance • Requires frequent dosing
• Offers potential for targeted
delivery
• Higher risk of side effects
• Flat line within therapeutic
range
• peaks and troughs
12.
Rationale for controlleddrug delivery system
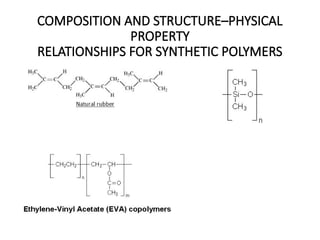
• The modified active moiety delivery technique is used to
improve bioavailability and to display therapeutic kinetics in
the body fluids.
• Modified therapeutic delivery technology is a composition
where the therapeutic candidate’s rate of release varies on
comparing to that of traditional dosage forms administered via
the similar mode of administration.
• The fundamental aim of this treatment was to maintain a
stable state of therapeutic concentration in blood or tissue for a
long time.
• The primary objective of controlled release system is to alter the
pharmacokinetic and pharmacodynamic characteristics of the
active therapeutic agent.
13.
Rationale for controlleddrug delivery system
• This might be accomplished by employing a new
medicinal delivery method or altering molecular
structure and physiological factors.
• A well-designed dosage form should last for a long
time. The primary objective of controlled release drug
delivery systems (CRDDS) is to secure the drug’s
safety profile while also increasing patient
compliance.
• Better management of plasma medication levels and
dosage frequency are used to accomplish this.
14.
• Sustained releasedrug
delivery is a method of
administering medication
that releases the drug
gradually over an extended
period, maintaining a
consistent drug level in the
body.
• This contrasts with
immediate-release
formulations, which
deliver the drug rapidly.
Sustained Release
15.
Classification of controlleddrug delivery system
• Controlled drug delivery systems
based on polymer membrane
permeability:
• The substance is stored within a
reservoir that is protected by
polymer membrane having
semipermeable characteristics
with a specific permeability that
regulates overall delivery of
active molecule
•
Rate-preprogrammed drug delivery systems:
16.
Classification of controlleddrug delivery system
• The pharmaceutical formulation is
encapsulated inside the reservoir
compartment forming nanospheres,
microsphere, hydrogel, thin layer
implants by spray coating,
microencapsulation, and many more
techniques.
• This system uses many drugs-related
factors like hydrophilic-lipophilic balance
and permeability, as well as rate-
controlling membrane-related parameters
like diameter of membrane, to govern the
distribution of bioactive compounds rate.
Rate-preprogrammed drug delivery systems:
17.
Classification of controlleddrug delivery system
• The substance is stored within a reservoir
that is protected by polymer membrane
having semipermeable characteristics with
a specific permeability that regulates
overall delivery of active molecule.
• The pharmaceutical formulation is
encapsulated inside the reservoir
compartment forming nanospheres,
microsphere, hydrogel, thin layer implants
by spray coating, microencapsulation, and
many more techniques.
Controlled drug delivery systems based on polymer membrane
permeability
18.
Classification of controlleddrug delivery system
• This system uses many drugs-
related factors like hydrophilic-
lipophilic balance and
permeability, as well as rate-
controlling membrane-related
parameters like diameter of
membrane, to govern the
distribution of bioactive
compounds at a predefined rate
Controlled drug delivery systems based on polymer membrane
permeability
19.
Classification of controlleddrug delivery system
• In this system, the biomolecules
are homogenously dispersed
with matrix polymer which can
be composed of water-soluble
polymer and/or oil-soluble
polymer.
• For instance, NitroDur is meant
to be applied to undamaged
skin for 24 h and deliver a
consistent transdermal infusion
of nitroglycerin
CRDDS -based polymer matrix diffusion:
20.
Classification of controlleddrug delivery system
• :It entails utilizing high energy
dispersion to disperse tiny particles of
medication solution (aqueous in
nature) in a polymer (silicone
elastomers).
• The dissolution- or matrix diffusion-
controlled release of drug molecules
from this sort of controlled release
drug delivery device is possible.
• Controlling various physicochemical
factors regulates the rate of release at
a predetermined pace. For example,
Syncromate implant—designed to
administer norgestomet through
subdermal injection
Controlled drug delivery systems based on micro reservoir partition
21.
Classification of controlleddrug delivery system
Rate preprogrammed drug delivery
system.
Activation modulated drug delivery
system
Feedback regulated drug delivery
system
Site targetting drug delivery system
RATE CONTROLLED DRUG DELIVERY SYSTEM
CLASSIFICATION
Classification of controlleddrug delivery system
• In this category, actives are delivered via drug carrier
that are triggered via stimulating element in the body,
such as a biological material, and are regulated by its
concentration via feedback mechanisms.
• The pace of medicine is controlled by the proportion of
stimulating element detected by a detector in this
system [9].
• The various designs are (1) bioerosion regulated DDS,
(2) bioresponsive DDS, and (3) self-regulated DDS.
Feedback-regulated drug delivery systems:
25.
Classification of controlleddrug delivery system
•
• It consists of a nonimmunogenic, biodegradable
polymer backbone with target groups which aids in
directing the drug carrier to the site-specific
cell/tissue/organ.
• Additionally, a solubilizer and drug molecules are also
present in system and works by allowing the carrier to
be transmitted to target site and exert therapeutic
effect, respectively.
Site-targeting drug delivery system:
Classification of controlleddrug delivery system
• Drug moiety covalently bonded to the polymer
backbone through a spacer.
• The rationale of site-specific delivery is to get
access to sites that were previously unreachable
(e.g., intracellular infections) and protection of
the medication and the body against undesired
deposits, which may have resulted in
unfavorable responses and metabolism, among
other things
Site-targeting drug delivery system:
28.
TERMINOLOGY
•
Prolonge
d release:
The medicationis delivered at a slow pace, but
over a longer length of time, allowing the
drug’s therapeutic effect to last longer.
Extended
release:
• The drug release is sustained over a long
stretch of time in extended release
formulations as they transit through the
gastrointestinal tract (GIT).
• Controlled release and sustained release are
two forms of extended release patterns with
different drug release rates.
• It is generally quicker at the start of the
releasing process and then gradually slows
down over time
29.
Terminology
•
Sustained
release:
• To maintainan adequate constant medication
concentration in the body over a long period of
duration, sustained release system will deliver the
biomolecules at predefined pace.
• The drug’s rate of release is governed by first-order
kinetics
Controlled
release:
• A controlled release system’s mission is to provide a
continual delivery of medicament, usually at a
constant order kinetics, through continuously
distributing a quantity of medicament proportionate
to amount eliminated from human system through
a specific period of time.
• An ideal system is one that delivers medications at a
predetermined rate, whether regionally or
systemically, for a predetermined period of time
30.
Terminology
•
Modified-
release
system:
• The term“modified-release drug product” refers to
drugs which alter the active ingredient’s release time
and/or rate.
• In this release system, the drug release characteristics of
duration and/or specific site are selected to satisfy
pharmacological effects beyond conventional system.
• Modified-release systems include delayed release (e.g.,
enteric coated), prolonged/extended release, and buccal
tablet form
Delayed
release
dosage
form:
• When a dosage form does not release the medication
immediately after administration, but instead releases it
in parts over time.
• Two types of delayed release dose forms are targeted
release and temporal delivery systems.
• Drug release is influenced by the gut environment,
including pH as well as enzymes present
31.
Targeted
drug
release
• This typeof delivery system includes the drug which
is given exclusively to the site of action and not to
nontargeted organs, tissues, or cells.
• The system is based on a technique that distributes
a specific quantity of a therapeutic substance to a
pathological region within the body over a
substantial amount of time, improving efficacy and
reducing adverse effects
Receptor
targeting
system
• In this approach, the substrate molecule will attach to
receptors that are abundantly present exclusively on
the targeted tissue or cell.
• Other typical cells will not have this sort of unique
receptor molecule.
• Furthermore, because they are expressed on the
surface of cells, they can be used as ligand directed
drug delivery targets.
•
Terminology
•
32.
Factors influencing designof CRDDS
• Drug-Related Factors
• Solubility: The drug's solubility in various media affects its
release rate.
• Partition coefficient: This determines the drug's distribution
between different phases, influencing release kinetics.
• Molecular weight and size: These factors affect the drug's
diffusion through the release system.
• Stability: The drug's stability under different conditions (pH,
temperature, humidity) is crucial for product shelf life.
• Therapeutic index: Drugs with a narrow therapeutic index
require precise control over drug release.
33.
Factors influencing designof CRDDS
• Patient-Related Factors
•Age: Physiological changes with age can affect
drug absorption and metabolism.
•Sex: Hormonal differences can influence drug
pharmacokinetics.
•Weight: Body weight can impact drug
distribution and elimination.
•Metabolism: Individual variations in
metabolism can affect drug clearance.
34.
Factors influencing designof CRDDS
• Patient-Related Factors
• Compliance: Patient adherence to the prescribed
dosing regimen is essential for CRDDS efficacy.
• Drug administration route determines the delivery
system's design (e.g., oral, transdermal,
injection).Target site dictates the release profile and
system's biocompatibility (e.g., local, systemic).
• Acute/chronic therapy influences the release rate and
duration (e.g., rapid release for acute, sustained release
for chronic).
• Disease characteristics determine the drug's
therapeutic index and required dosing regimen,
impacting system design.
36.
Factors influencing designof CRDDS
• Therapeutic Considerations
• Desired therapeutic effect: The intended therapeutic outcome
dictates the release profile.
• Dosing regimen: The desired dosing frequency and duration influence
the CRDDS design.
• Therapeutic window: Drugs with a narrow therapeutic window
require precise control over drug release.
• Formulation Factors
• Polymer type and properties: The polymer used in the CRDDS affects
the drug release rate.
• Excipients: Additives can influence drug release, stability, and product
characteristics.
• Manufacturing process: The production method affects the final
product's properties.
37.
Factors influencing designof CRDDS
• Regulatory Factors
• Safety and efficacy: The CRDDS must meet stringent regulatory
requirements for safety and efficacy.
• Bioequivalence: The product must demonstrate bioequivalence to the
reference product.
• Stability and shelf life: The CRDDS must maintain its quality and
potency throughout its shelf life.
• Other Factors
• Cost-effectiveness: The development and production costs of the
CRDDS should be considered.
• Patient acceptance: The product's size, shape, and administration
method should be acceptable to patients.
• Environmental impact: The environmental impact of the CRDDS and
its production process should be minimized.
38.
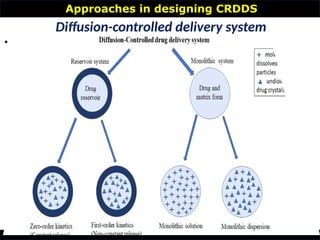
Approaches in designingCRDDS
•
Diffusion-controlled delivery system
1.Diffusional mass transfer is mostly including
the delivery of therapeutic molecule from the
formulation.
2.Drug diffusion is the primary step in certain
situations and also a rate-limiting factor.
3.The release rate of a drug in a diffusional
system is determined by its diffusion through
an inert membrane barrier.
4.This barrier is usually of an insoluble polymer.
39.
Approaches in designingCRDDS
•
Diffusion-controlled delivery system
5. The basic notion is that an active molecule
diffuses out of the dosage form and the
principle mechanism involves the movement
of that active compound from the region of
high concentration to that of the lower
concentration.
6. Fick’s first law of diffusion states that flux
J is proportional to the diffusivity(D) and
the negative gradient of concentration ,
ϕ
when diffusion occurs in a single direction,
x
Approaches in designingCRDDS
•
Diffusion-controlled delivery system
This equation tells us that the rate of change of concentration at a
particular point (∂C/∂t) is proportional to the curvature of the
concentration gradient (∂²C/∂x²).
If the concentration gradient is steep (high curvature), the
concentration will change rapidly. This means the substance will
diffuse quickly to areas of lower concentration.
If the concentration gradient is shallow (low curvature), the
concentration will change slowly. Diffusion will occur more
gradually.
Zero vs Firstorder
•
Diffusion-controlled delivery system
1.
44.
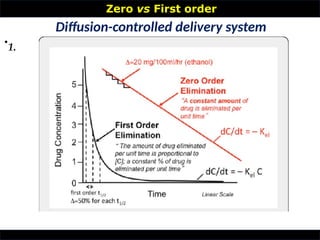
Zero vs Firstorder
•
Monolithic matrix system
• Drug molecules are evenly distributed throughout the nonporous,
water-insoluble polymer matrix in monolithic devices.
• Unlike reservoir devices, these system lacks the outer coat
polymeric layer.
• These monolithic systems have no risk of drug dumping, resulting
in no small flaws because of the absence of outer polymeric coat
around the core moiety.
• Furthermore, they are less expensive to manufacture and easier to
build than reservoir devices.
• They are characterized by the active agent being placed directly
homogenized in polymeric matrix, which helps in storing the drug
and aids in diffusion at required site thus, avoid the difficulties
associated with reservoir systems.
• Prior to performing the diffusion to the surface, the matrix must
first be dissolved. As a result, the delivery behavior from this type
of system is somewhat different from the reservoir and other types
of mechanism
45.
Zero vs Firstorder
•
Dissolution CRDDS
• Because the rate of dissolution will restrict the
amount of drug released, it appears self-evident that
the therapeutic moiety bearing slow-going
dissolution kinetics might have prolonged release
characteristics for designing CRDDS.
• When the rate of dissolution is high, the drug is
combined with a slow-dissolving carrier and a
tablet is created to maintain or regulate the drug’s
release.
• The pace at which a medicament goes into the
solution is employed in estimation of the drug
releasing from the therapeutic carrier system
46.
Zero vs Firstorder
•
Dissolution CRDDS
• When the exterior region of the delivery device
releases the initial dose of the drug quickly, the initial
concentration of the drug is rapidly reached, followed
by predetermined period of time gap.
• Although this may be not included as the basic
controlled release drug formulation, the
pharmaceutical and biological properties of the drug
are often comparable
Another option for the drug delivery is administering
the molecule of interest in the form of several bunch of
rounded beads with varying polished thicknesses,
allowing for progressive drug release. The thinnest layer
will deliver the initial dose.
47.
Zero vs Firstorder
•
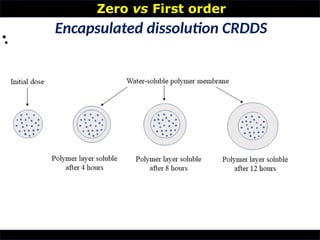
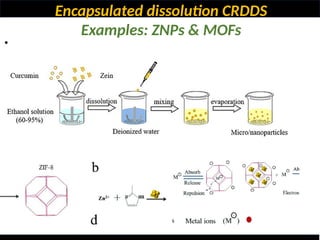
Encapsulated dissolution CRDDS
• Density of coated layer and disintegration of coated
polymeric layer governs the release kinetics of drug
molecules in this system.
• Therefore full chemical moiety is immediately
accessible for dissolving and absorption once the
coated polymer membrane dissolves.
• The size of solute particles can affect the release
kinetics of drug.
• The formulation bearing different solute particles will
show the release behavior differently.
• After the formulation administration, the thickness of
the polymeric coating increases with respect to time
48.
Zero vs Firstorder
•
Encapsulated dissolution CRDDS
•
•
Matrix dissolution CRDDS
ZIF-8
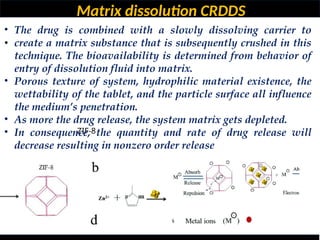
•The drug is combined with a slowly dissolving carrier to
create a matrix substance that is subsequently crushed in this
technique. The bioavailability is determined from behavior of
entry of dissolution fluid into matrix.
• Porous texture of system, hydrophilic material existence, the
wettability of the tablet, and the particle surface all influence
the medium’s penetration.
• As more the drug release, the system matrix gets depleted.
• In consequence, the quantity and rate of drug release will
decrease resulting in nonzero order release
51.
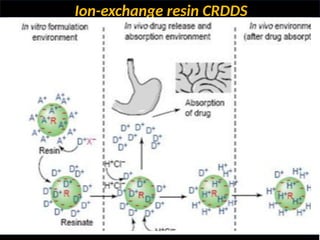
Ion-exchange resin CRDDS
ZIF-8
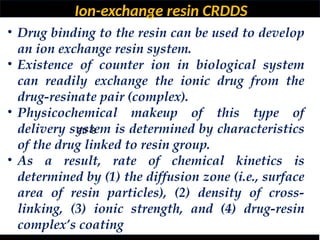
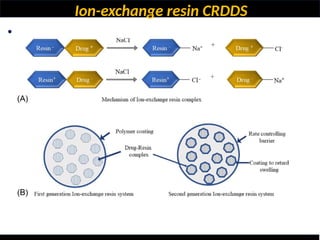
•Drug binding to the resin can be used to develop
an ion exchange resin system.
• Existence of counter ion in biological system
can readily exchange the ionic drug from the
drug-resinate pair (complex).
• Physicochemical makeup of this type of
delivery system is determined by characteristics
of the drug linked to resin group.
• As a result, rate of chemical kinetics is
determined by (1) the diffusion zone (i.e., surface
area of resin particles), (2) density of cross-
linking, (3) ionic strength, and (4) drug-resin
complex’s coating
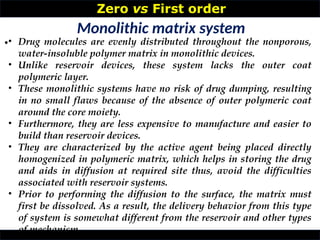
Osmotic CRDDS
ZIF-8
• Osmotic-controlledrelease preparations are
becoming increasingly important for the
advancement in technology of various
formulations, owing to their capacity to
distribute pharmaceuticals uniformly at
consistent rate throughout the period of time,
regardless of any external factors like fluid
dynamics, temperature, pH [71,72].
• The preparation consisted of an active
substance containing core, a semipermeable
layer which coats the solid drug moiety at the
center and aperture created an orifice allowing
the therapeutic moiety to escape
55.
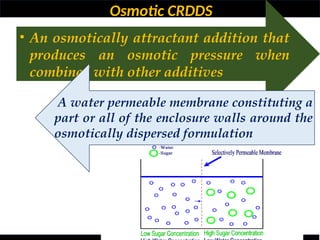
Osmotic CRDDS
• Anosmotically attractant addition that
produces an osmotic pressure when
combined with other additives
A water permeable membrane constituting a
part or all of the enclosure walls around the
osmotically dispersed formulation
56.
Water is osmotically
pulledinto the enclosure
when put in an aqueous
environment by the
combined action of the
active component and the
moveable partition, which
swells up, and delivers the
active substance from the
orifice into external
environment
57.
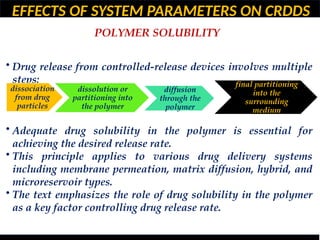
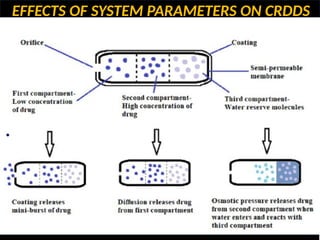
EFFECTS OF SYSTEMPARAMETERS ON CRDDS
• Drug release from controlled-release systems is influenced
by various factors.
• Key factors affecting drug release include partition
coefficient, diffusivity, solubility, and membrane thickness.
• Different drug delivery systems (membrane permeation,
matrix diffusion, hybrid, microreservoir) have varying
degrees of dependence on these factors.
• The study emphasizes the importance of understanding
these system parameters for effective drug delivery system
design.
58.
EFFECTS OF SYSTEMPARAMETERS ON CRDDS
POLYMER SOLUBILITY
• Drug release from controlled-release devices involves multiple
steps:
• Adequate drug solubility in the polymer is essential for
achieving the desired release rate.
• This principle applies to various drug delivery systems
including membrane permeation, matrix diffusion, hybrid, and
microreservoir types.
• The text emphasizes the role of drug solubility in the polymer
as a key factor controlling drug release rate.
dissociation
from drug
particles
dissolution or
partitioning into
the polymer
diffusion
through the
polymer
final partitioning
into the
surrounding
medium
59.
EFFECTS OF SYSTEMPARAMETERS ON CRDDS
SOLUTION SOLUBILITY
•
• Medium Type: Norgestral and megestrel acetate
released faster in plasma than in distilled water.
• Protein Binding: Steroids released 2-15 times faster
in human plasma than normal saline due to
increased solubility from protein binding.
• Solution Solubility (Cs): This factor plays a crucial
role in determining drug release rate from drug
delivery systems.
• Medium Volume: Reducing the volume of distilled
water decreased progesterone release by 50%.
60.
EFFECTS OF SYSTEMPARAMETERS ON CRDDS
How Polymer Solubility Affects Drug Release
•
WATER-SOLUBLE POLYMERS:
• Swelling and erosion: These polymers absorb
water, swell, and form a gel-like matrix.
• The drug diffuses through this matrix.
• Example: Hydroxypropyl methylcellulose (HPMC)
is commonly used in matrix tablets for sustained
release.
• Drug release rate: Generally slower due to the
diffusional barrier created by the swollen polymer.
61.
EFFECTS OF SYSTEMPARAMETERS ON CRDDS
How Polymer Solubility Affects Drug Release
•
WATER-INSOLUBLE POLYMERS
Diffusion:
The drug diffuses through the polymer matrix, which
does not dissolve in water.
Example: Ethyl cellulose is used in many controlled
release formulations.
Drug release rate: Can be controlled by polymer
thickness, porosity, and drug solubility in the
polymer..
62.
EFFECTS OF SYSTEMPARAMETERS ON CRDDS
How Polymer Solubility Affects Drug Release
•
PARTIALLY SOLUBLE POLYMERS
Combination of swelling and erosion:
These polymers exhibit properties of both water-
soluble and water-insoluble polymers.
Example: Cellulose acetate phthalate (CAP) is a pH-
dependent polymer used in enteric coatings.
Drug release rate: Can be modulated by pH changes
in the gastrointestinal tract.
63.
EFFECTS OF SYSTEMPARAMETERS ON CRDDS
How Polymer Solubility Affects Drug Release
•
Matrix tablets:
HPMC-based matrix tablets for sustained release of
theophylline.
Ethyl cellulose-based matrix tablets for controlled
release of nifedipine.
Coated tablets:
Enteric-coated tablets using CAP for delayed release
in the small intestine.
Polymer-coated pellets with varying polymer
thicknesses for multiphasic release.
64.
EFFECTS OF SYSTEMPARAMETERS ON CRDDS
How Polymer Solubility Affects Drug Release
•
Osmotic systems:
Semipermeable membranes made of water-insoluble
polymers control drug release.
Example:
OROS (Osmotic Controlled Release Oral Delivery
System)system for controlled release of nifedipine.
EFFECTS OF SYSTEMPARAMETERS ON CRDDS
PARTITION COEFFICIENT
•
• The partition coefficient (K) is a crucial parameter
in the design of controlled release drug delivery
systems.
• It represents the ratio of a drug's solubility in the
elution solution (Cs) to its solubility in the
polymer composition (Cp) of the drug delivery
device.
• A higher partition coefficient generally leads to a
faster drug release rate.
67.
EFFECTS OF SYSTEMPARAMETERS ON CRDDS
PARTITION COEFFICIENT
•
• This is because the drug has a greater affinity for
the elution medium, promoting its diffusion out of
the system.
• Conversely, a lower partition coefficient results in
a slower release rate as the drug is more inclined to
remain within the polymer matrix.
• Drug Loading: The partition coefficient influences
the amount of drug that can be loaded into the
system.
• A higher K allows for higher drug loading, while a
lower K limits the amount of drug that can be
incorporated.
68.
EFFECTS OF SYSTEMPARAMETERS ON CRDDS
Polymer Selection:
•
• The choice of polymer for the drug delivery system
is influenced by the drug's partition coefficient.
• Polymers with higher affinity for the drug (lower
K) can be used to achieve sustained release profiles.
System Design:
• The overall design of the drug delivery system,
including its geometry, size, and coating, can be
optimized based on the drug's partition coefficient
to achieve the desired release profile.
69.
EFFECTS OF SYSTEMPARAMETERS ON CRDDS
•
• Predictability of Release Profiles:
Understanding the partition coefficient helps in
predicting the release behavior of a drug from a
given system, enabling better control over drug
delivery.
70.
Impact of PolymerDiffusivity on Controlled
Release Drug Delivery System Design
•
•
• Drug Release Rate:
• Higher diffusivity: Leads to faster drug release as molecules
can move more rapidly through the polymer.
• Lower diffusivity: Results in slower drug release, providing a
sustained release profile.
• Release Kinetics:
• Fickian diffusion: Predictable release profile where the drug
release rate is proportional to the concentration gradient.
• Non-Fickian diffusion: Complex release behavior influenced
by factors like polymer swelling or relaxation, leading to
varying release rates.
71.
Impact of PolymerDiffusivity on Controlled
Release Drug Delivery System Design
•
•
• Polymer Selection:
• Polymers with high diffusivity are suitable for
immediate or rapid release formulations.
• Polymers with low diffusivity are preferred for
sustained or controlled release systems.
• System Geometry:
• The shape and size of the drug delivery system can
influence the diffusion path length, affecting drug
release rate.
• For instance, a thin film will allow for faster diffusion
compared to a thick matrix.
72.
Impact of PathLength on Controlled Release
Drug Delivery System Design
•
•
•
How Path Length Affects Drug Release:
•Longer path length:
•Slower release: As the drug molecules have to travel a
greater distance to reach the surrounding medium, the
release rate is reduced.
•More sustained release: Longer path lengths often result
in a more sustained release profile.
•Shorter path length:
•Faster release: Drug molecules can escape more quickly,
leading to a faster initial release rate.
•Less sustained release: Shorter path lengths often result
in a less sustained release profile.
73.
Examples of Impactof Path Length on
Controlled Release Drug Delivery System
Design
•
•
•
•Matrix systems:
• Increasing the thickness of the polymer matrix increases
the path length, leading to slower drug release.
• Using a more permeable polymer can reduce the
effective path length, increasing drug release rate.
•Coated systems:
• The thickness of the coating determines the path length
for drug diffusion.
• Thicker coatings result in slower release, while thinner
coatings allow for faster release.
74.
Examples of Impactof Path Length on
Controlled Release Drug Delivery System
Design
•
•
•
Practical Implications:
•Sustained release: By increasing the path length,
drug release can be prolonged, reducing dosing
frequency.
•Controlled release: By carefully adjusting the path
length, drug release can be tailored to specific
therapeutic needs.
•Zero-order release: Achieving a constant drug release
rate often requires careful control of the path length.
75.
Impact of PolymerDiffusivity on Controlled
Release Drug Delivery System Design
•
•
• Drug Loading:
• Higher drug loading can impact polymer diffusivity,
potentially leading to changes in release kinetics.
• By carefully selecting polymers with appropriate
diffusivity and modifying system parameters, desired
release profiles can be achieved.
•
76.
Strategies to ModifyPolymer Diffusivity
•
•
• Polymer Blending: Combining polymers with
different diffusivities can create systems with
tailored release profiles.
• Crosslinking: Increasing polymer crosslinking
reduces diffusivity, leading to slower release.
• Porosity: Introducing pores into the polymer matrix
can enhance diffusivity.
• Polymer Molecular Weight: Higher molecular
weight polymers generally exhibit lower diffusivity.
77.
EVALUATION
•
•
• Understand drugrelease mechanisms: Investigate how the
drug is released from the dosage form (e.g., diffusion, erosion,
osmotic pressure).
• Assess drug release kinetics: Determine the rate and pattern
of drug release over time.
• Predict in vivo performance: Correlate in vitro release data
with in vivo pharmacokinetic parameters to anticipate the drug's
behavior in the body.
• Optimize formulation: Refine the dosage form's composition
and design to achieve the desired release profile.
• Ensure product quality and consistency: Monitor batch-to-
batch variability and detect any changes in drug release
characteristics.
78.
EVALUATION
•
•
• Understand drugrelease mechanisms: Investigate how the
drug is released from the dosage form (e.g., diffusion, erosion,
osmotic pressure).
• Assess drug release kinetics: Determine the rate and pattern
of drug release over time.
• Predict in vivo performance: Correlate in vitro release data
with in vivo pharmacokinetic parameters to anticipate the drug's
behavior in the body.
• Optimize formulation: Refine the dosage form's composition
and design to achieve the desired release profile.
• Ensure product quality and consistency: Monitor batch-to-
batch variability and detect any changes in drug release
characteristics.
over the dosage form, providing a more dynamic environment.
d by measuring the drug concentration in the surrounding medium.
79.
EVALUATION
•
•
• In VitroRelease Studies:
• Determine the drug release profile under controlled conditions.
• Assess factors like drug loading, polymer type, and system geometry.
• Evaluate the release kinetics (zero-order, first-order, etc.) to
understand the release mechanism.
•In Vivo Studies:
• Pharmacokinetic studies to assess drug absorption, distribution,
metabolism, and elimination.
• Pharmacodynamic studies to evaluate the therapeutic efficacy and
safety of the system.
• Biodistribution studies to determine drug concentration in target
tissues.
•Stability Studies:
• Evaluate the system's stability under various storage conditions
(temperature, humidity, light).
• Assess drug degradation and changes in release profile over time.
80.
PK OF CRDDS
Absorption
•
•
•Prolonged Absorption: Instead of a rapid burst of drug, CRDDS release the drug
slowly and continuously over an extended period. This leads to a more uniform
and prolonged absorption phase.
• Maintenance of Therapeutic Levels: By providing a consistent drug
concentration at the absorption site, CRDDS help maintain plasma drug levels
within the therapeutic window for longer durations, avoiding the "peak and
valley" fluctuations seen with conventional dosing. This minimizes both sub-
therapeutic levels and toxic peaks.
• Reduced Dosing Frequency: Due to extended absorption, CRDDS reduce the
need for frequent drug administration, improving patient compliance.
• Improved Bioavailability (for some drugs): For drugs that are unstable in certain
parts of the GI tract (e.g., acidic stomach) or are extensively metabolized in the
gut wall (first-pass metabolism), controlled release can bypass these issues by
delivering the drug to more favorable absorption sites or by slowing the release to
prevent saturation of metabolic enzymes.
81.
PK OF CRDDS
Distribution
•
•
•Consistent Plasma Levels: By maintaining more uniform plasma
concentrations, CRDDS can lead to more stable drug distribution to
target tissues, potentially optimizing the therapeutic effect.
• Reduced Fluctuation in Tissue Levels: The steady supply of drug
from CRDDS minimizes large fluctuations in drug concentration in
various tissues, which can be beneficial for drugs requiring sustained
levels at the site of action.
• Localized Delivery: Some CRDDS are designed for targeted or local
delivery (e.g., implants, ocular inserts). In these cases, distribution is
highly localized, maximizing drug concentration at the desired site
while minimizing systemic exposure and associated side effects.
82.
PK OF CRDDS
Metabolism
•
•
•Reduced First-Pass Metabolism (for some drugs): By slowing down
the rate of absorption, CRDDS can prevent the saturation of
metabolizing enzymes in the gut wall or liver, potentially increasing
the systemic bioavailability of drugs that undergo extensive first-pass
metabolism.
• Sustained Enzyme Exposure: For drugs metabolized by inducible
enzymes, prolonged exposure from CRDDS might lead to sustained
enzyme induction or inhibition, altering their metabolic profile over
time.
• Potential for Increased Degradation: If a drug is unstable in the GI
tract or susceptible to enzymatic degradation in the lumen or gut
wall, a prolonged residence time due to controlled release might
theoretically expose it to more degradation, potentially decreasing
83.
PK OF CRDDS
Elimination
•
•
•ProlongedElimination Phase:
Since the drug is absorbed over a longer period, the "apparent"
half-life might appear longer than the true biological half-life,
as drug continues to be released into the system while it's also
being eliminated. This contributes to the extended duration of
action.
Steady-State Considerations:
For drugs administered repeatedly, CRDDS help in achieving
and maintaining steady-state plasma concentrations more
smoothly and for longer periods with less fluctuation, making
dosing regimens simpler.
85.
IVIVC in controlledrelease
•
•
• In Vitro Release Studies:
• Determine the drug release profile under controlled conditions.
• Assess factors like drug loading, polymer type, and system geometry.
• Evaluate the release kinetics (zero-order, first-order, etc.) to
understand the release mechanism.
•In Vivo Studies:
• Pharmacokinetic studies to assess drug absorption, distribution,
metabolism, and elimination.
• Pharmacodynamic studies to evaluate the therapeutic efficacy and
safety of the system.
• Biodistribution studies to determine drug concentration in target
tissues.
•Stability Studies:
• Evaluate the system's stability under various storage conditions
(temperature, humidity, light).
• Assess drug degradation and changes in release profile over time.
EVALUATION
•
•
Correlation with InVivo Performance
• While in vitro studies provide valuable information, it's
important to recognize that they don't perfectly predict in
vivo performance.
• Factors such as gastrointestinal physiology, metabolism,
and drug distribution can influence drug absorption and
bioavailability.
• Therefore, in vivo studies are ultimately required to
confirm the clinical efficacy and safety of CRDFs.
88.
EVALUATION
•
•
•
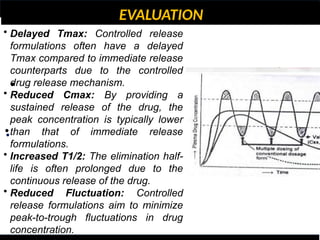
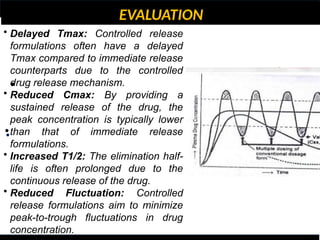
• Delayed Tmax:Controlled release
formulations often have a delayed
Tmax compared to immediate release
counterparts due to the controlled
drug release mechanism.
• Reduced Cmax: By providing a
sustained release of the drug, the
peak concentration is typically lower
than that of immediate release
formulations.
• Increased T1/2: The elimination half-
life is often prolonged due to the
continuous release of the drug.
• Reduced Fluctuation: Controlled
release formulations aim to minimize
peak-to-trough fluctuations in drug
concentration.
89.
EVALUATION
•
•
•
• Delayed Tmax:Controlled release
formulations often have a delayed
Tmax compared to immediate release
counterparts due to the controlled
drug release mechanism.
• Reduced Cmax: By providing a
sustained release of the drug, the
peak concentration is typically lower
than that of immediate release
formulations.
• Increased T1/2: The elimination half-
life is often prolonged due to the
continuous release of the drug.
• Reduced Fluctuation: Controlled
release formulations aim to minimize
peak-to-trough fluctuations in drug
concentration.
90.
Conclusion
ZIF-8
• Drug deliverycarriers have significantly
advanced in recent decades.
• These carriers enhance drug potency and safety
through controlled release.
• Scientists focus on designing local drug delivery
devices.
• Understanding release mechanisms, drug
properties, and barriers is crucial.
• The primary goal is to deliver the right drug, in
the right amount, to the right place.
• Various factors influence the development of
controlled release drug delivery systems
(CRDDS).
An intraocular lens(IOL) must be
transparent and dimensionally stable.
Protein and lipid
absorptions are issues that also should
be probed, but only after selecting a
group of
materials for an IOL that are
transparent and dimensionally stable
93.
• The ballin a ball-in-cage heart valve must be both
dimensionally and mechanically stable during the cyclic
movements up against the top of the metal stents and
back down to the bottom of the cage where it must
make a good seal.
• A related, key factor is that the ball should absorb
minimal amounts of water or lipids, which would
change both its dimensions and mechanical properties.
Blood compatibilities are a secondary concern for this
application, because the patient will probably have to
take an anticoagulant drug on a chronic basis.
94.
• Blood oxygenatormembrane must have good
permeability to oxygen and CO2 .
• Blood interactions are secondary here especially as
the patient’s blood is probably going to be
anticoagulated with heparin during bypass
oxygenation.
95.
• Dental cementmust have good adhesive
properties, both to the surfaces of the tooth and to
the filling material, and must be water resistant
once cured. If the cement is going to be subjected
to chewing stresses, then both the adhesive bond
strength and cohesive strength under cyclic
compressive stresses will be critical to the success
of a dental cement. Protein adsorption or bacterial
adhesion are not critical.
96.
• A drugdelivery device or system must release the
drug at the desired rate, and in order for clinical
success, the polymer components of the delivery
vehicle must swell (or not), or degrade (or not), or
dissolve (or not), or be retrieved (if necessary) after
the drug is depleted. The demands on these key
properties of the polymer components of a drug
delivery system are critical to its success.
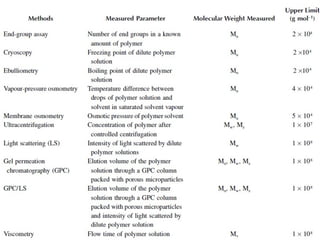
LIGHT SCATTERING
• Whena parallel beam of light passes through a transparent system, a small part of the
light is scattered elastically (Rayleigh scattering).
• The scattering arises because of optical discontinuities in the medium.
• For solutions of polymer molecules, additional scattering arises from the presence of
the solute molecules, and this may be shown to be a function of the concentration of
the polymer molecules, as well as their size and shape.
• When measurements are made of the differences in intensity of the scattered light
between the solvent and a series of dilute polymer solutions, then it is possible to
determine the averaged size of polymer solutes and hence their molecular weights.
• The results of the measurement are usually expressed as the weight-average molecular
weight.
• The theoretical basis of light scattering from polymer solutions was first established by
107.
GEL PERMEATION CHROMATOGRAPHY
•GPC or size exclusion chromatography (SEC) is a very convenient and
simple way of measuring polymer molecular weights and the
distribution of these values about their mean.
• The polymer solution is injected into a solvent stream that flows
through one or more columns packed with highly porous
microparticles, and polymer molecules are separated according to
their size.
• The small molecules enter the deep pores, and their progress is
retarded relative to the large molecules.
• Detection of the polymer mass in the eluent is accomplished using
either a refractive index (RI) or ultraviolet absorption (UV) detector.
• The RI detector detects solutes based on the difference between the
refractive index of the solution and the solvent, and the UV detector
detects solutes based on their absorption of light of a particular
wavelength.
VIBRATIONAL SPECTROSCOPY —
INFRAREDAND RAMAN SPECTROSCOPY
• This method has been extensively applied to
characterize the polymer’s molecular and material
structure.
• An example of its use is for the determination of the
level of amine groups in chitosan.
• Chitosan is an increasingly interesting polysaccharide in
the drug delivery field, and the amine content of
chitosan is very important for various applications. The
absorption band ratios of amide II at 1655 cm−1
to the
hydroxyl group at 3450 cm−1
, i.e., A1655/A3450, has been
used for amine content determination.
110.
3.4 NUCLEAR MAGNETICRESONANCE
SPECTROSCOPY
• NMR is a most powerful tool for the study of the microstructure and chain
configuration of polymers, both in solution and in the solid state.
• The importance of NMR as a technique stems from the fact that the NMR signals can
be assigned to specific atoms along the polymer backbone and side chains.
• The identification of certain atoms or groups in a polymer molecule as well as their
positions relative to each other can be obtained by one-, two- and three-dimensional
NMR spectra [1,8,9].
• The NMR technique utilizes the property of spin possessed by nuclei such as 1H, 13C,
15N, 17O, and 19F.
• When a strong external magnetic field (the strength H0 is at least 10,000 G) is applied
to
• material containing such nuclei, they behave like bar magnets and can orientate
themselves in two
• energy states, a low-energy state, in which the alignment is parallel to the field, and a
high-energy
• state, in which the alignment is opposed to the field
111.
OPTICAL MICROSCOPY
• Opticalmicroscopy provides microstructural information with a
resolution on the order of 1 μm.
• Imaging is carried out using both reflected and transmitted light. If
the absorption coefficient varies
• regionally within a sample, when a beam of light travels through
such a sample, contrasting regions
• of intensity will be obtained in the final image. For a specimen that
can be prepared as a thin film,
• for instance, by casting on the microscope slide, examination using
transmitted light is most useful,
• but little detail can be observed without some type of contrast
enhancement. Two common techniques
• available to achieve contrast are polarized-light microscopy and
phase-contrast microscopy
112.
TRANSMISSION ELECTRON MICROSCOPY
•Transmission electron microscopy (TEM) involves transmitting a beam
of electrons instead of light
• through a sample in a high-vacuum environment. The images and
associated contrasts arise from
• regional differences in electron densities. TEM has a resolution of
about 1 to 100 nm, and it can
• thus provide very detailed structural information on polymeric
materials, even down to the molecular
• level.
113.
SCANNING ELECTRON
MICROSCOPY
• Scanningelectron microscopy (SEM) is another very valuable electron
microscopy technique with a
• resolution of about 5 nm. In SEM, a fine beam of electrons is scanned across
the surface of an opaque
• specimen, and an appropriate detector collects the electrons emitted from
each point. In this way, an
• image having a great depth of field and a remarkable three-dimensional
appearance is built up line
• by line. To produce stable images, the specimen is usually coated with a
conducting film prior to
• examination. In most cases, a gold or gold–palladium alloy is used to coat the
surface either by
• evaporation or by sputtering. The typical film thickness is about 20 nm.
Another advantage of coating
• is that coating materials can give a high secondary electron yield and thus
increase image contrast.
114.
THERMAL GRAVIMETRY
• 3.6.2This method is used to measure the change in weight of a
polymer sample while it is heated, using
• a sensitive balance. Such a weight change would indicate a physical
or chemical change in the
• material and is used for the characterization of drug-containing
polymeric materials.
115.
MECHANICAL AND
RHEOLOGICAL ANALYSES
•The mechanical and rheological properties of polymers are a reflection of the polymers’
molecular
• (molecular weight, molecular weight distribution, conformation, architecture, and
crystallinity)
• properties. An assessment of a polymer’s mechanical and rheological properties is often
carried
• out in order to establish if the polymer is fit for the purpose [8].
• The tensile properties of solid polymers can be characterized by their deformation
behavior,
• which is obtained by measuring stress–strain responses. Rubbery polymers are soft and
reversibly
• extensible and exhibit a lower modulus or stiffness. Glass and semicrystalline polymers
have higher
• moduli and lower extensibility. If network structures are achieved from the cross-linking of
polymers,
• large-scale movement or flow is prevented, because the freedom of motion of the polymer
• chain is restricted [13].

![• Controlled drug delivery systems can help retain drug levels
within a certain range, reduce the dosing frequency, maximize
the effectiveness of the medicine, and improve patient
compliance [1].
• The most essential and frequent justification for their appeal
is the ease to be administered. Carry-ability and
manufacturing on a large scale are both straightforward.
• Two criteria would be necessary if one needs to envision the
optimum drug delivery system. Initially, the dose for the
entire course of treatment should be solitary and especially
for the chronic ailments, as in the case of hypertension or
diabetes.
• Secondly, the delivery of active ingredient should be site
specific, thereby eliminating the toxicity for other
organs/tissues
Controlled Release…](https://image.slidesharecdn.com/controlledreleasedds-250818105108-c72b567c/85/CONTROLLED-RELEASE-drug-delivery-systems-4-320.jpg)

![Classification of controlled drug delivery system
• In this category, actives are delivered via drug carrier
that are triggered via stimulating element in the body,
such as a biological material, and are regulated by its
concentration via feedback mechanisms.
• The pace of medicine is controlled by the proportion of
stimulating element detected by a detector in this
system [9].
• The various designs are (1) bioerosion regulated DDS,
(2) bioresponsive DDS, and (3) self-regulated DDS.
Feedback-regulated drug delivery systems:](https://image.slidesharecdn.com/controlledreleasedds-250818105108-c72b567c/85/CONTROLLED-RELEASE-drug-delivery-systems-24-320.jpg)


![Osmotic CRDDS
ZIF-8
• Osmotic-controlled release preparations are
becoming increasingly important for the
advancement in technology of various
formulations, owing to their capacity to
distribute pharmaceuticals uniformly at
consistent rate throughout the period of time,
regardless of any external factors like fluid
dynamics, temperature, pH [71,72].
• The preparation consisted of an active
substance containing core, a semipermeable
layer which coats the solid drug moiety at the
center and aperture created an orifice allowing
the therapeutic moiety to escape](https://image.slidesharecdn.com/controlledreleasedds-250818105108-c72b567c/85/CONTROLLED-RELEASE-drug-delivery-systems-54-320.jpg)


![3.4 NUCLEAR MAGNETIC RESONANCE
SPECTROSCOPY
• NMR is a most powerful tool for the study of the microstructure and chain
configuration of polymers, both in solution and in the solid state.
• The importance of NMR as a technique stems from the fact that the NMR signals can
be assigned to specific atoms along the polymer backbone and side chains.
• The identification of certain atoms or groups in a polymer molecule as well as their
positions relative to each other can be obtained by one-, two- and three-dimensional
NMR spectra [1,8,9].
• The NMR technique utilizes the property of spin possessed by nuclei such as 1H, 13C,
15N, 17O, and 19F.
• When a strong external magnetic field (the strength H0 is at least 10,000 G) is applied
to
• material containing such nuclei, they behave like bar magnets and can orientate
themselves in two
• energy states, a low-energy state, in which the alignment is parallel to the field, and a
high-energy
• state, in which the alignment is opposed to the field](https://image.slidesharecdn.com/controlledreleasedds-250818105108-c72b567c/85/CONTROLLED-RELEASE-drug-delivery-systems-110-320.jpg)
![MECHANICAL AND
RHEOLOGICAL ANALYSES
• The mechanical and rheological properties of polymers are a reflection of the polymers’
molecular
• (molecular weight, molecular weight distribution, conformation, architecture, and
crystallinity)
• properties. An assessment of a polymer’s mechanical and rheological properties is often
carried
• out in order to establish if the polymer is fit for the purpose [8].
• The tensile properties of solid polymers can be characterized by their deformation
behavior,
• which is obtained by measuring stress–strain responses. Rubbery polymers are soft and
reversibly
• extensible and exhibit a lower modulus or stiffness. Glass and semicrystalline polymers
have higher
• moduli and lower extensibility. If network structures are achieved from the cross-linking of
polymers,
• large-scale movement or flow is prevented, because the freedom of motion of the polymer
• chain is restricted [13].](https://image.slidesharecdn.com/controlledreleasedds-250818105108-c72b567c/85/CONTROLLED-RELEASE-drug-delivery-systems-115-320.jpg)