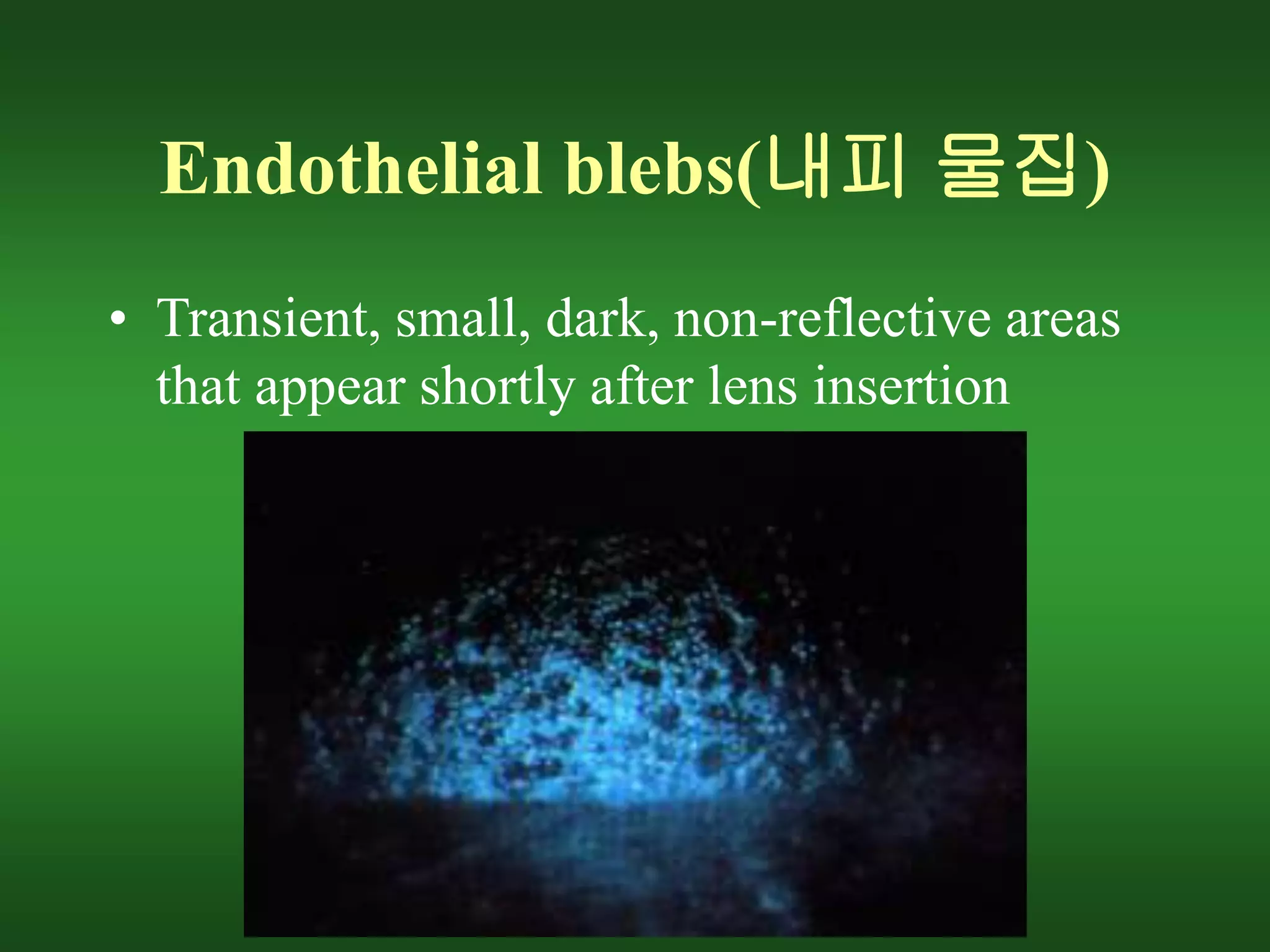
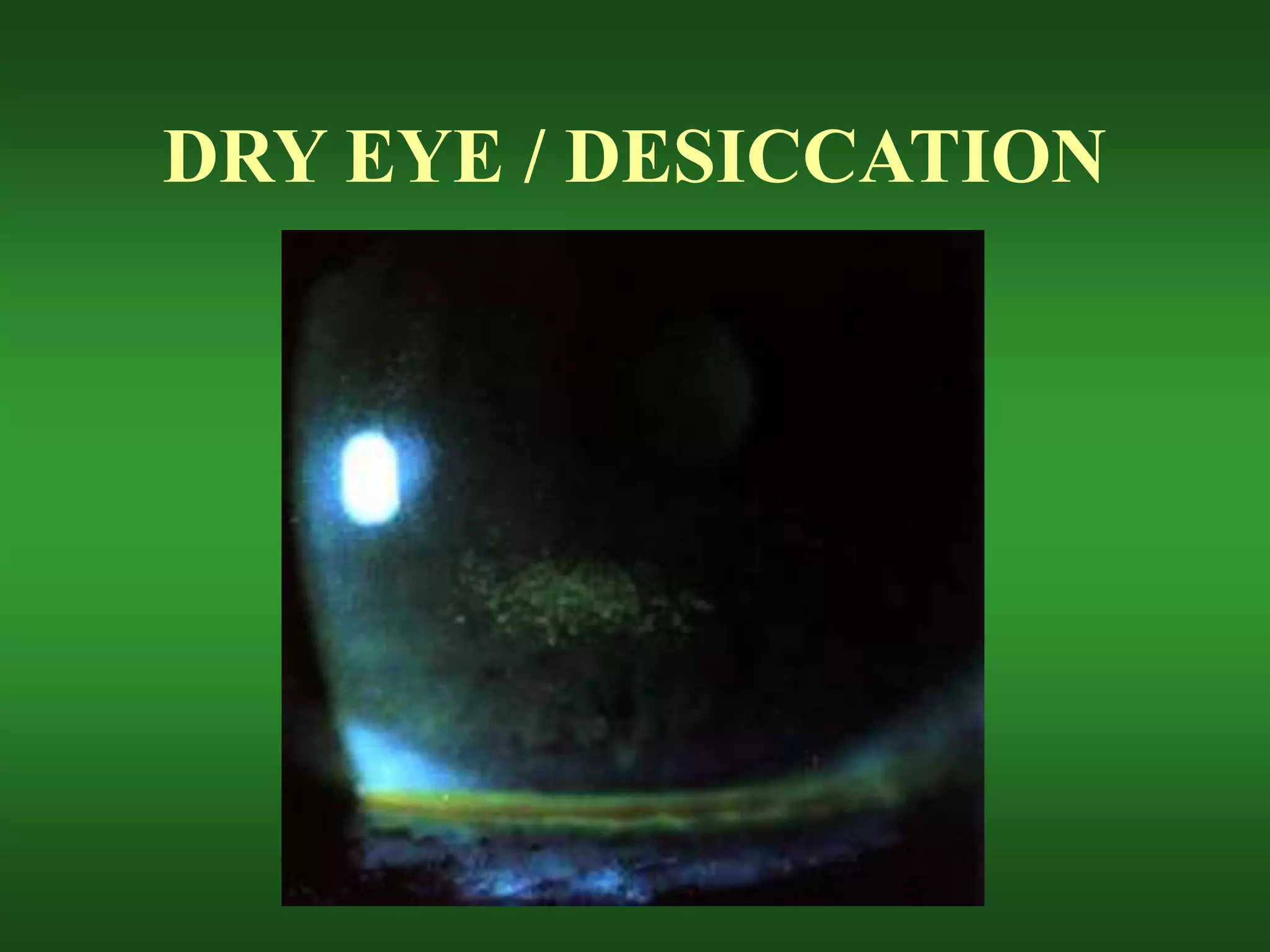
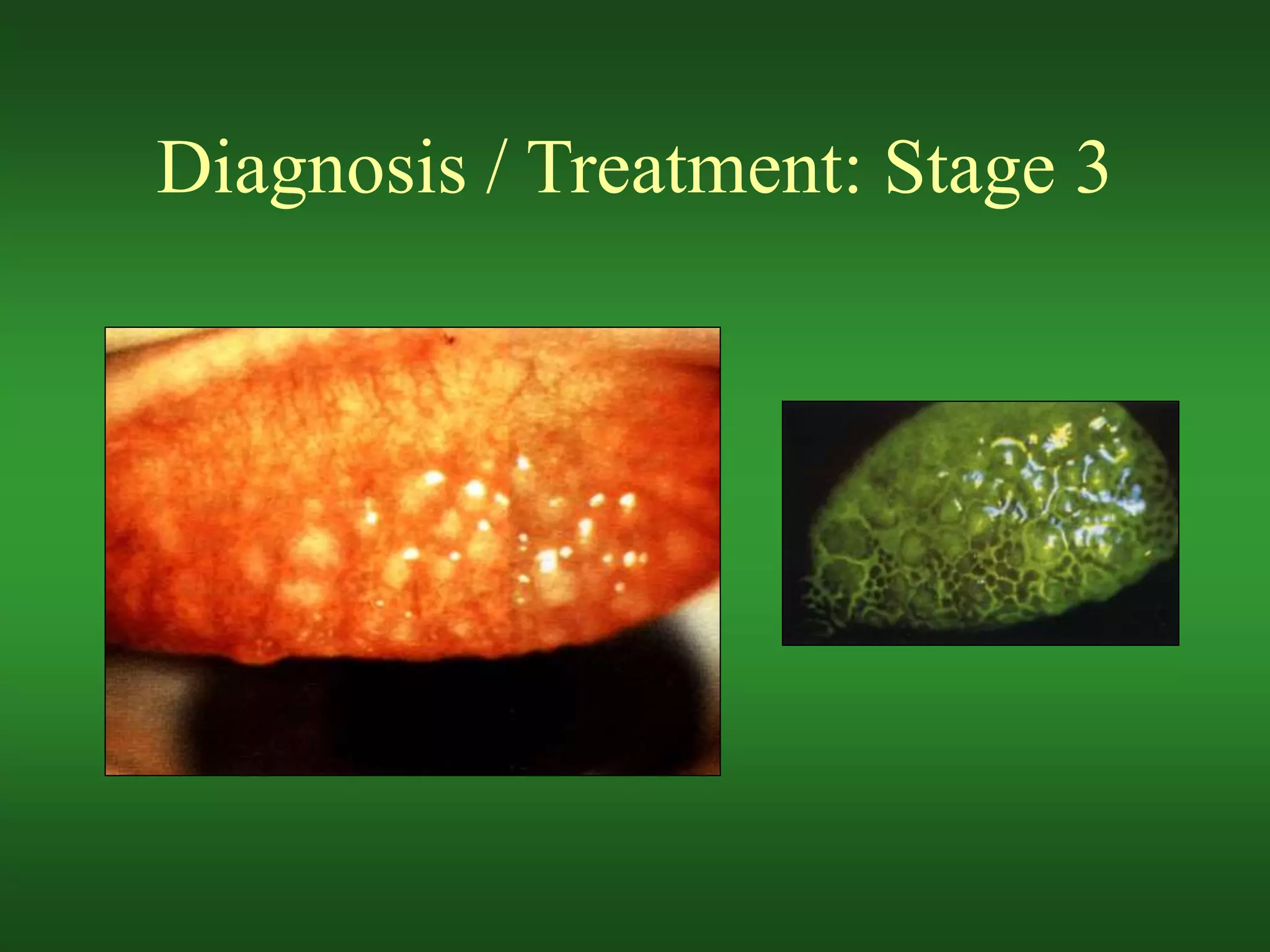
The document discusses various risks and complications that can arise from soft contact lens wear, including hypoxia, desiccation, deposit buildup, mechanical issues, and inflammatory responses. It covers specific conditions like epithelial edema, stromal edema, microcysts, vascularization, polymegethism, endothelial blebs, dry eye, contact lens papillary conjunctivitis, contact lens superior limbic keratoconjunctivitis, acute red eye, sterile infiltrates and ulcers, and preservative allergies and sensitivities. Potential causes, symptoms, diagnoses, and treatment approaches are provided for each condition.