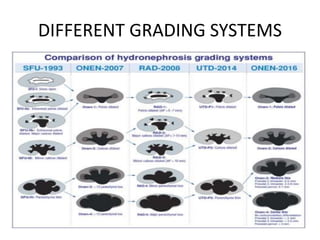
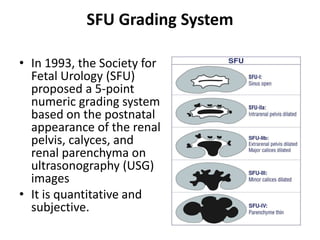
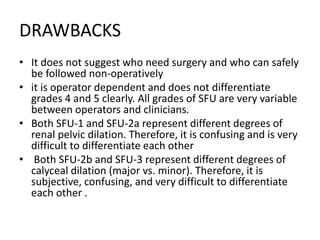
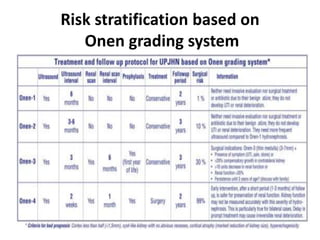
This document discusses different grading systems used to evaluate congenital hydronephrosis seen on ultrasound imaging. It outlines systems like the SFU grading scale and radiology grading scale but notes limitations in reliability between observers. The Onen grading system is presented as having clear terminology to classify dilation of the pelvicalyceal system and quality of renal parenchyma. The document concludes by proposing a risk stratification system for congenital hydronephrosis based on the Onen grading scale to determine need for early surgical intervention or likelihood of resolution.





































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)









![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)



