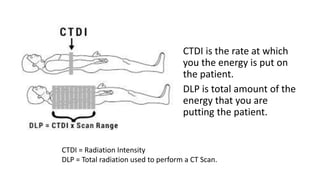
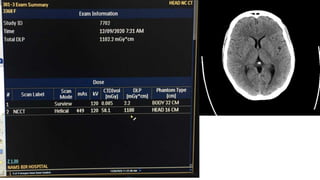
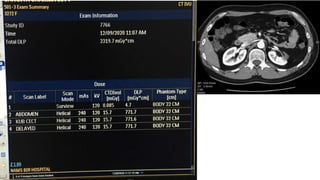
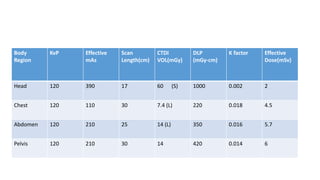
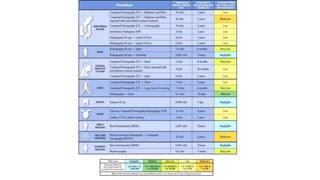
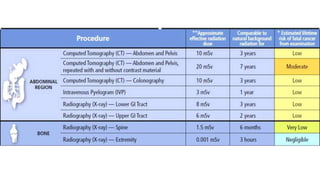
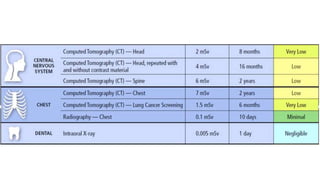
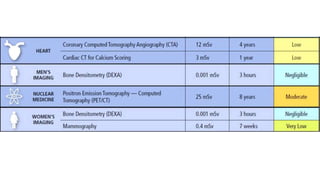
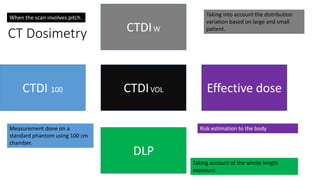
The document discusses the measurement of radiation dose in computed tomography (CT), highlighting concepts like absorbed dose, effective dose, and the differences between deterministic and stochastic effects of radiation. It explains the use of standard phantoms for estimating patient doses, the relationship between CT parameters such as CTDI and DLP, and the methods for calculating effective doses using Monte Carlo simulations. Additionally, it outlines how to account for tissue sensitivity and variations in patient anatomy in dose measurements.