Downloaded 53 times
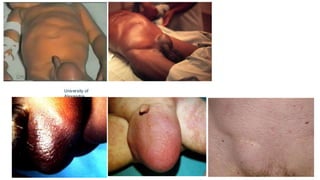
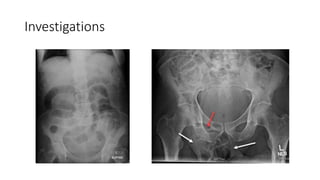
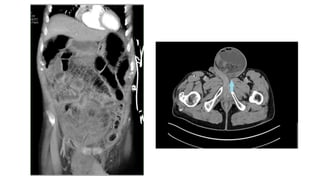
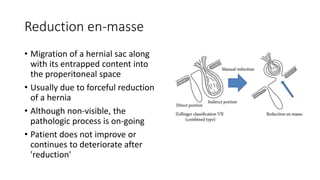

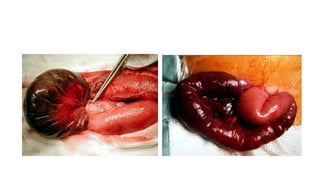

The document discusses complicated hernias, including their definition, epidemiology, classification, clinical presentation, investigations, and treatment options. It highlights the differing presentations and complications of groin hernias, including femoral and obturator hernias, and emphasizes the importance of surgical intervention in cases of obstruction or strangulation. The management of hernias involves careful investigation, resuscitation, and potentially laparoscopic or open surgical repair, particularly in emergency situations.














































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)






![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)

