Downloaded 53 times

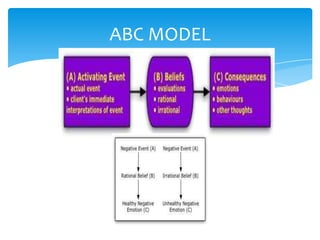
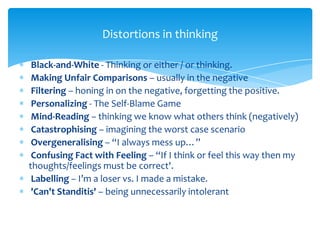
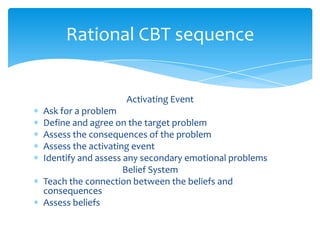
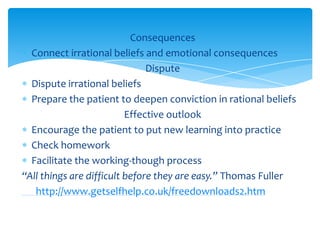
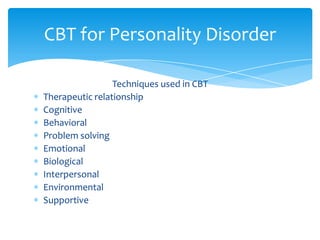
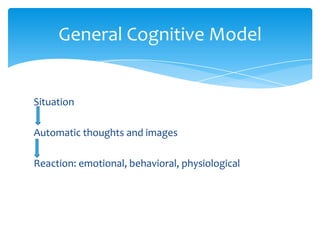
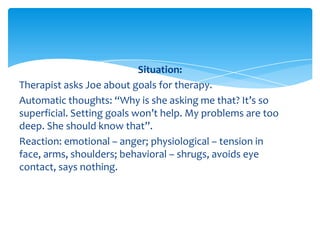
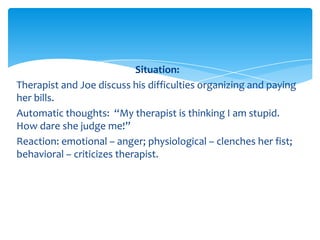

The document discusses cognitive behavioral therapy (CBT) and mindfulness. It provides objectives and content for a presentation on these topics, including definitions of CBT and mindfulness, models like ABCDE that are used in CBT, and techniques involved. The role of mindfulness in developing acceptance is explained. Examples are given of how to apply CBT models to specific situations. Core beliefs and developing new beliefs are also addressed.























































































