Downloaded 201 times















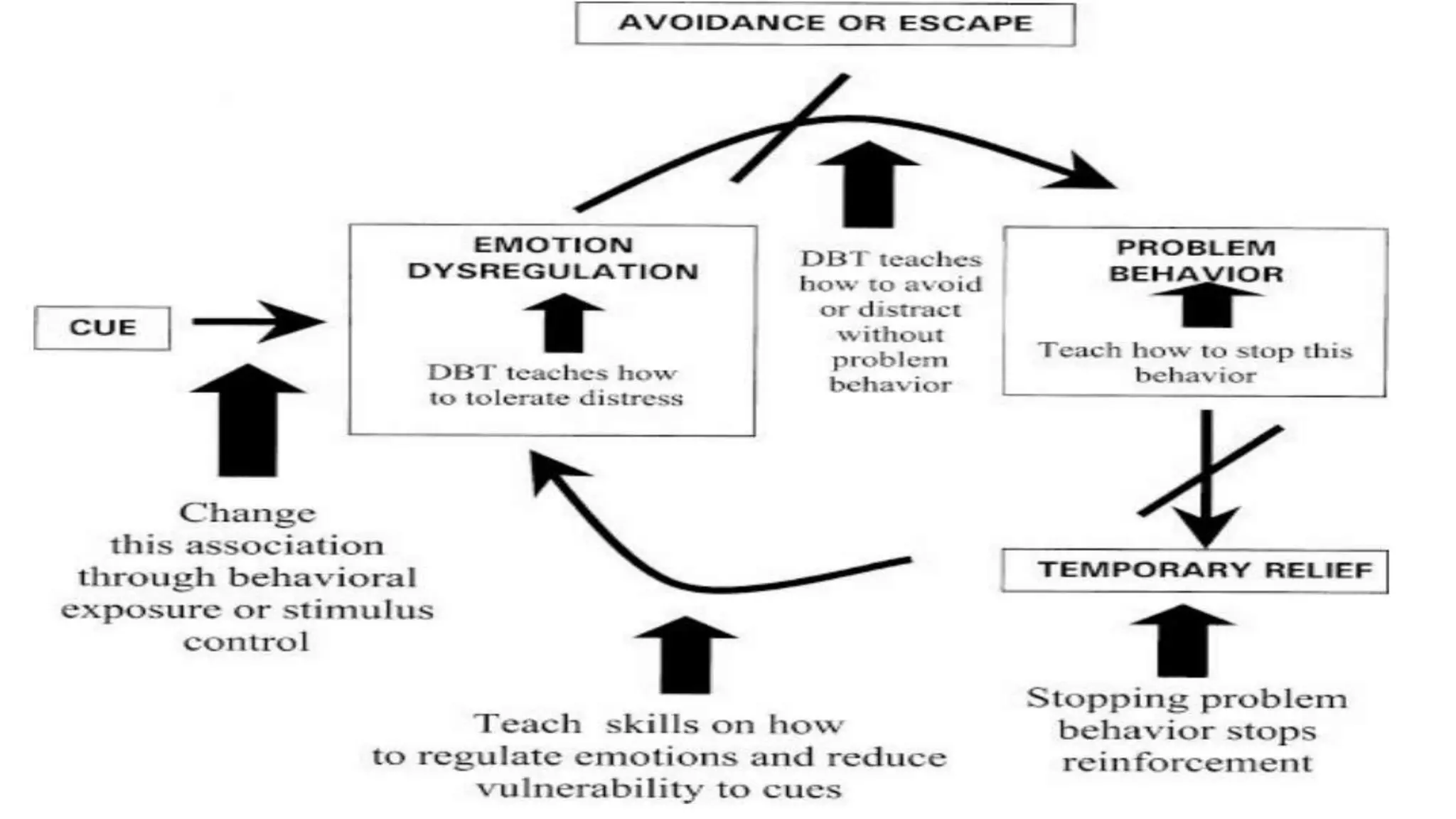



Dialectical Behavior Therapy (DBT) is a cognitive-behavioral treatment developed to treat borderline personality disorder. It uses individual therapy, group skills training, telephone coaching, and a therapist consultation team. DBT aims to help patients manage emotions and impulses through mindfulness, distress tolerance, emotion regulation, and interpersonal effectiveness skills. Studies have found DBT reduces self-harm behaviors and improves social and work functioning for patients with borderline personality disorder.












































































