CHRONIC MYELOID LEUKAEMIA
BY;
U19MD2013,U19MD2014, U19MD2015, U19MD2016,U19MD2017
U19MD2018, U19MD2019, U19MD2020
Department of Haematology and Blood Transfusion
Faculty of Basic Clinical Sciences College of Medical
Sciences Ahmadu Bello University Zaria
MODERATORS: Prof. Aliyu A. Babadoko, Prof. AM. Sulaiman,
Dr. Garba
Date: 25/11/2024
2.
OUTLINE
● Introduction
● DefineChronic myeloid Leukaemia
● Describe the aetiological factors for CML
● Pathogenesis of Chronic Myeloid Leukaemia
● Clinical features
● Investigations
● Describe the phases of Chronic Myeloid Leukaemia
● Treatment and follow-up
● Mode of action of Imatinib Mesylate (Glivec)
● Clinical Scenario
3.
INTRODUCTION
Leukemia is acancer of the blood forming cells
araising from the bone marrow and is characterized
by increase in the number of White blood cells
(leucocytes) in the peripheral blood or bone marrow
4.
DEFINITION
Chronic myelogenous leukemia(CML) Is a clonal
myeloproliferative disorder of the pluripotent hematopoietic stem
cell characterized by increase proliferation of the granulocytic cell
line without the loss of their capacity to differentiate. The
peripheral blood cells profile shows an increased number of
granulocytes and their immature precursors and may include
blasts
5.
AETIOLOGICAL FACTORS
The aetiologicalfactors for CML primarily revolve around genetic
and environmental influences, with the hallmark being the
presence of the Philadelphia chromosome (Ph chromosome). The
following are overview of its key aetiological factors:
6.
GENETIC FACTORS
● PhiladelphiaChromosome: CML is almost universally
associated with the Philadelphia chromosome, a result of the
reciprocal translocation between chromosomes 9 and 22,
t(9;22)(q34;q11)
● Stochastic Events: CML may also arise due to random
genetic mutations during hematopoietic stem cell division,
independent of identifiable environmental or inherited
factors
7.
ENVIRONMENTAL FACTORS
Radiation Exposure:,
●Ionizing radiation: Exposure to high levels of ionizing radiation, such
as from nuclear accidents or radiation therapy, increases the risk of
developing CML
Chemical Exposure:,
● Benzene: Exposure to benzene, a chemical commonly used in
industrial processes, has been linked to an increased risk of
developing CML
● Pesticides and herbicides: Some studies suggest that exposure to
certain pesticides and herbicides may increase the risk of
developing CML
8.
AGE AND DEMOGRAPHICFACTORS
● Age: CML is more common in adults, with the majority of
cases diagnosed between the ages of 50 and 70. The risk
increases with age
● Sex: CML is slightly more common in males than females
● Familial Risk: While CML is not typically inherited, rare
familial clusters suggest a possible genetic predisposition
9.
OTHER FACTORS
● Smoking
●Sporadic: Majority of CML cases occur without a clear cause
or risk factor
● Multiple factors: CML results from a combination of genetic
environmental, and lifestyle factors
10.
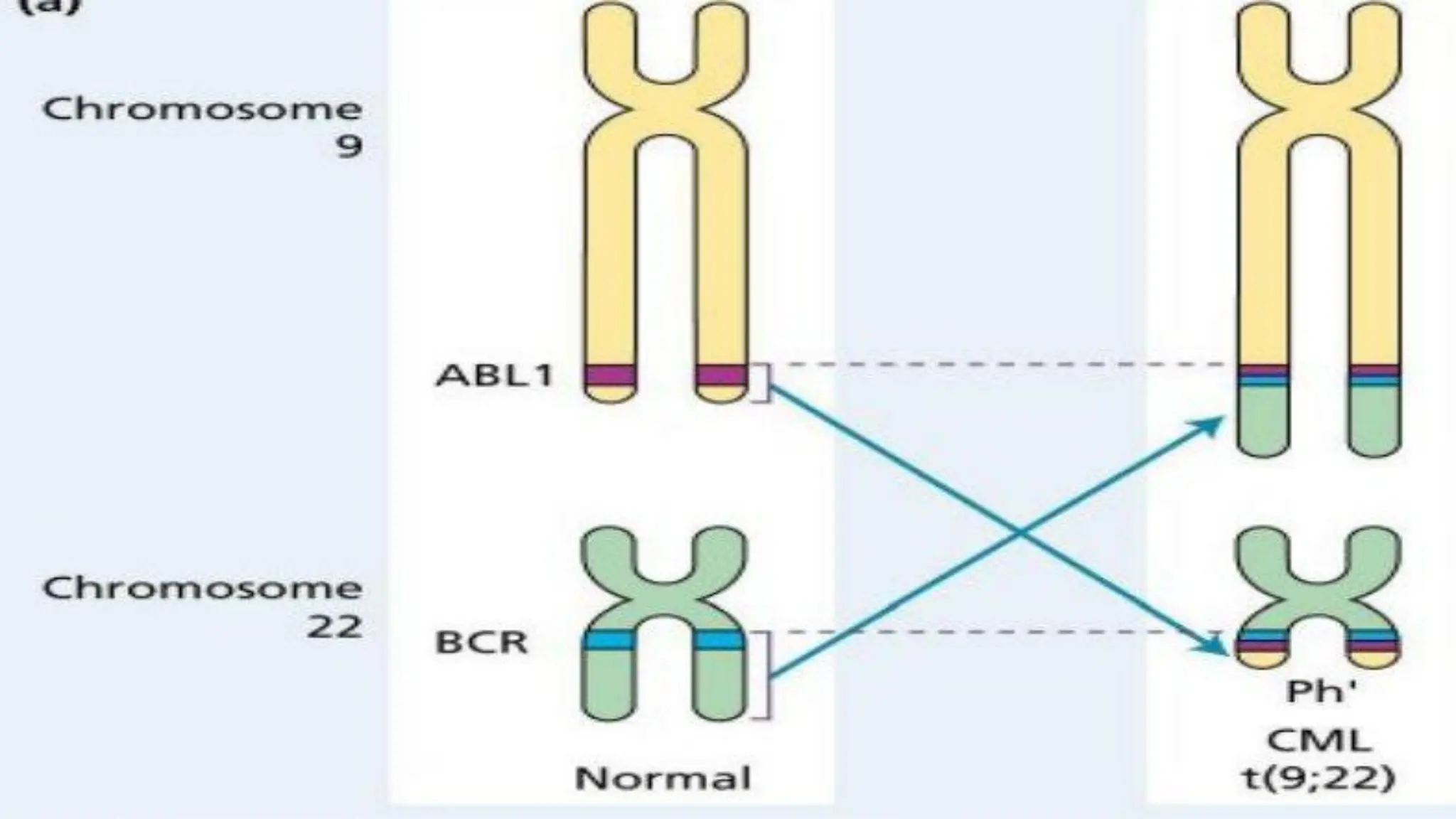
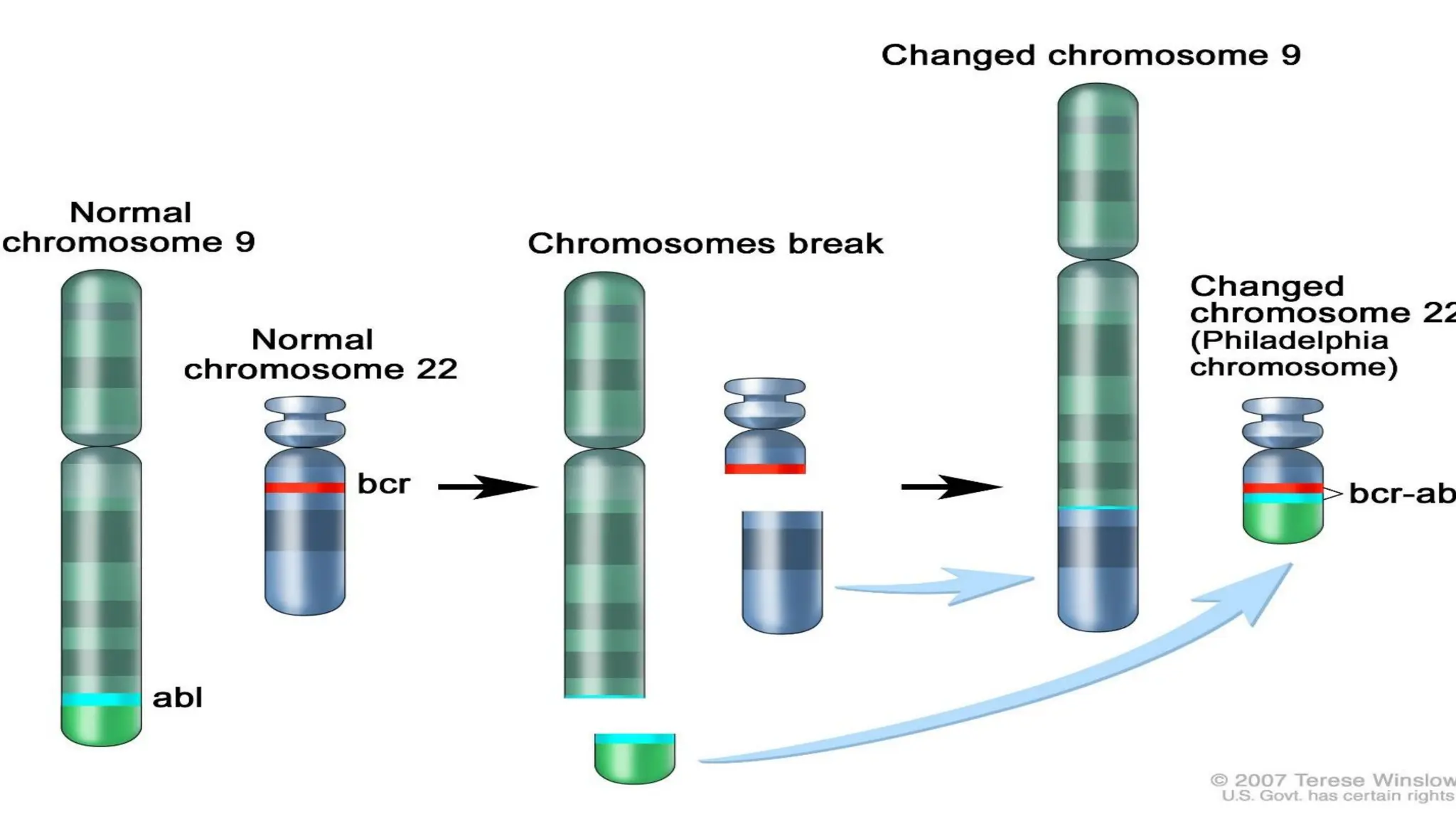
PATHOGENESIS
● CML ischaracterized by the presence of a distinct molecular
abnormality referred to as Philadelphia (Ph) chromosome
● It is formed as a result of reciprocal translocation of genetic
material between the long arms of one chromosome 22 and one
chromosome t(9;22) (q34;q11)
● The translocation involves the BCR gene on chromosome 9 and
the ABL gene on chromosome 22
● The resultant BCR/ABL chimeric fusion gene directs the synthesis
of a protein with tyrosine kinase activity
● This active TK is confined to the cytoplasm
11.
PHATO. CONT.
● TheTK activity resides in ABL protein with juxtaposition of
BCR sequences next to ABL
● The site of breakpoint in BCR gene varies from 185 kDa to
230 kDa
● Most patients with typical CML have 210 kDa fusion protein
12.
PHATO. CONT.
● TheBCR/ABL protein activates a number of cytoplasmic and
nuclear signal transduction pathways
● This activation affects cell growth and differentiation
● Uncontrolled activity of TK ultimately results in deregulation
of cellular proliferation, decreased apoptosis and poor
adherence of leukaemic cells to BM stroma
14.
PHATO. CONT.
● Itstimulates cell cycle entry of haemopoietic cell lines in the
absence of growth factors
● It reduces the expression of cell surface adhesion molecules,
thereby
● facilitating the dissemination of leukaemic cells in the
peripheral blood
● It allows leukaemic cells to evade apoptosis
15.
PHATO. CONT
● Itallows leukaemic cells to evade apoptosis
● The Ph chromosome is present in all myeloid cell lineages
● In some B-cells and a few proportions of T-cells
● There are 3 forms of the BCR/ABL mutation
● p190, p210, p230 (they all have increased TK activity)
17.
CLINICAL FEATURES
Symptoms andSigns
● Patients are often asymptomatic early on, with insidious onset
of nonspecific symptoms (e.g. fatigue, weakness, anorexia,
weight loss, fever, night sweats, a sense of abdominal
fullness), which may prompt evaluation
● Initially, pallor, bleeding, easy bruising, and lymphadenopathy
are unusual
18.
CLINICAL FEATURES. CONT.
Somepatients present with splenomegaly and this is usually
massive and features relating to the splenomegaly such as:
•easy satiety
•dragging sensation in the abdomen
•Left upper quadrant pain from the splenomegaly or even
•splenic infarct
19.
CLINICAL FEATURES. CONT
Occasionallypatients may present with hyperleukostasis due to
severe leukocytosis or thrombosis. Presentations may include:
•vaso occlusive disease
•CVA
•MI
•venous thrombosis
•priapism
• visual disturbance
•Auditory disturbances
•pulmonary insufficiency
20.
CONT.
Progression of CMLis associated with worsening of symptoms,
such as:
•unexplained fever
•significant weight loss
•bone and joint pain
•bleeding
•thrombosis
This may suggests transformation into accelerated or blastic
phase
21.
CONT.
Histamine production 2⁰to basophil increase in later stage causing
•pruritus
•diarrhoea and
• flushing
•hepatomegaly may be noted
•Discrete masses of immature leukaemic cells may be seen in the skin
and other tissues ,and are sometimes called granulocytic sarcoma
(chloroma, extramedullary myeloid tumor)
22.
INVESTIGATION
FBC;
● PCV -Low
● WBC counts- Leucocytosis may reach >200*10⁹/L
● Platelets count- may be normal, increase or decrease
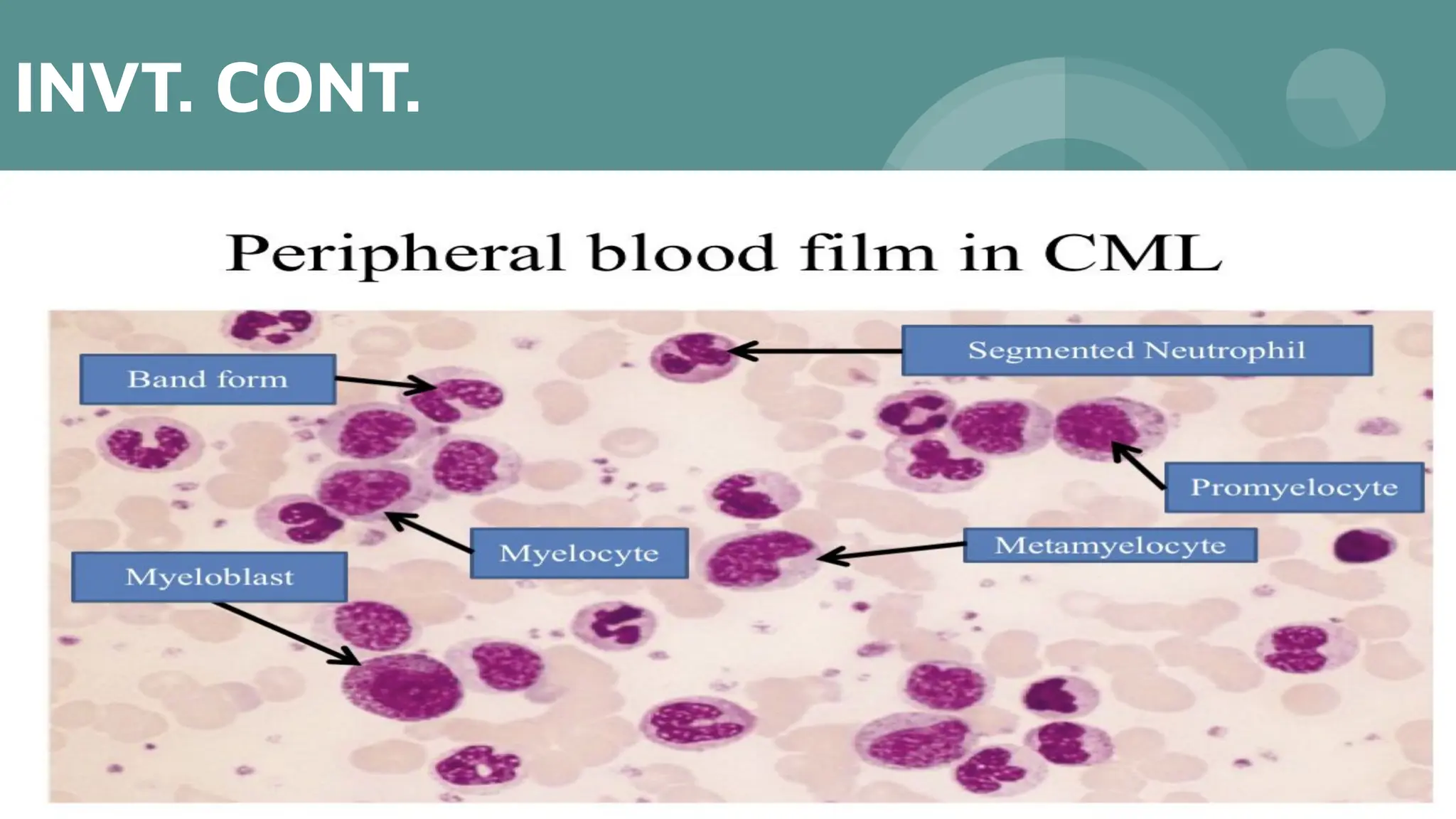
Blood FIlm;
● RBC- Normocytic normochromic
● WBC-Blood picture show a full spectrum of cells in the
granulocytic series ranging from blasts form to mature
neutrophils with myelocytes
INVT. CONT.
Bone marrowexamination;
● Hypercellular with granulocytic predominance and <10%
myeloblast
● Megakaryocytes increase and dysplastic
Cytogenetic analysis of BM;
● Philadelphia chromosome
● Reciprocal transportation t(9;22) in >95% of cases
Molecular analysis of BM;
● BCR-ABL by FISH or PCR in 100% of cases
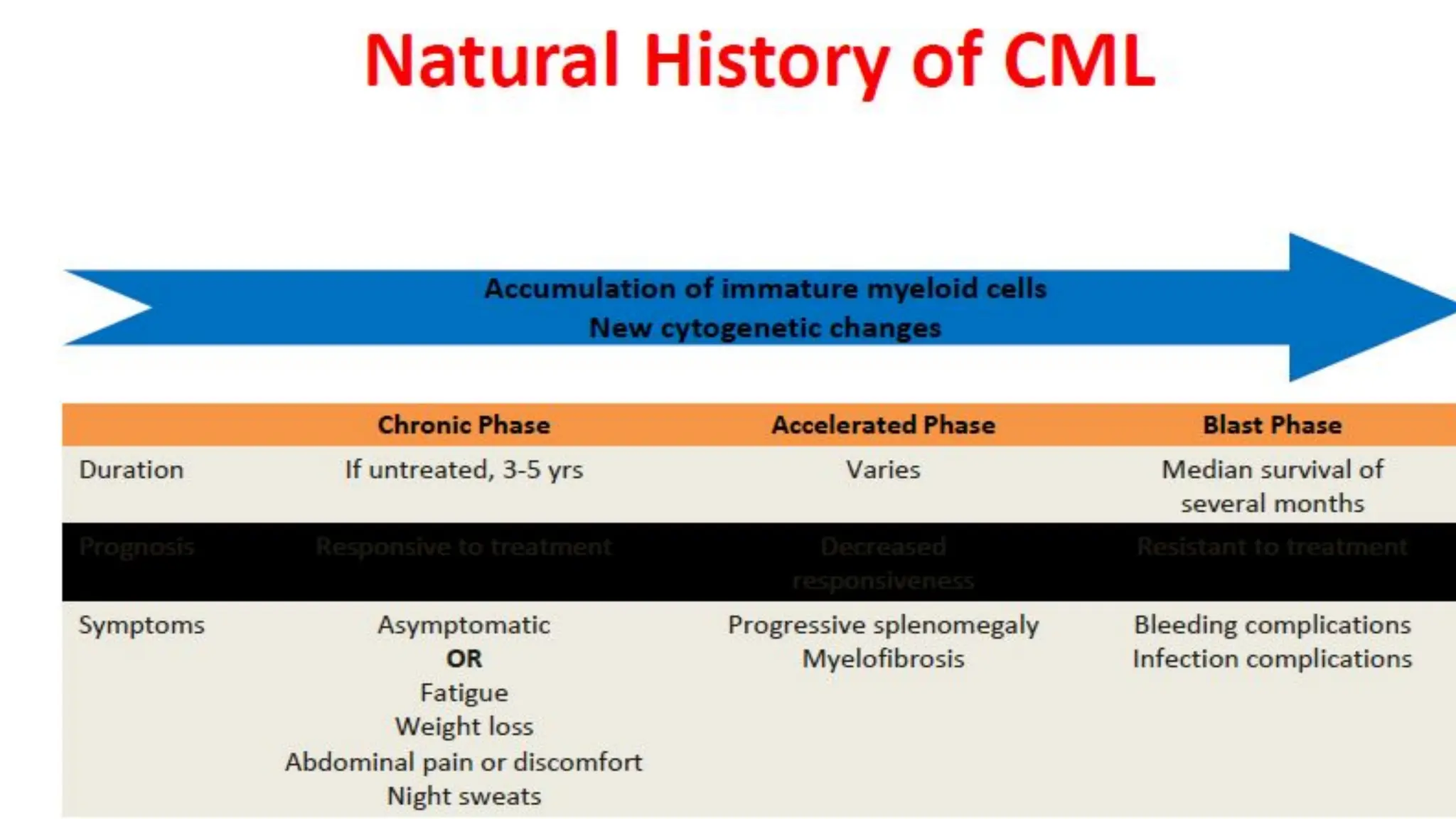
PHASES OF CML
●The clinical course of CML is usually biphasic or triphasic.
● Characterized by chronic stable phase which progresses to a more
aggressive phase and eventually to blastic phase
Chronic phase
● Diagnosis is made at this phase in 85% of cases
● The leukemic cells retain the capacity for differentiation and
maturation and they are largely able to function normally
● There is gradual increase in WBC, splenic enlargement and B
symptoms
27.
● Duration ofchange from the stable disease is variable
● May present in accelerated phase without clear chronic
phase
Accelerated phase
● About 70% progresses to accelerated phase
● There is increase proliferation and loss of maturation
● Leukocytes counts are more difficult to control with
myelosuppressive drugs
● Becomes resistance to chemotherapy
● Persistent or increasing splenomegaly
● Increase immature granulocytes in blood
28.
● The diseasebecomes more aggressive and further mutation
or clonal evolutions
● About 30% progresses to blastic phase within few months
WHO criteria for accelerated phase
Presence of one or more of the following features
● Increased percentage of blast cells(10-19%) in the
peripheral blood and or bone marrow
● Persistent thrombocytopenia unresponsive to therapy
● Progressive splenomegaly and increase in leukocyte count
despite treatment
● Cytogenetic evidence of clonal evolution
29.
Blastic phase
● Characterizedby presence of more than 20% of leukemic
blasts or
● Blast plus promyeloblast in the peripheral blood or bone
marrow
● The transformation could either be myeloid (70%) or
lymphoid(30%)
● Additional non random chromosomal abnormalities occur
during evolution to blastic transformation
30.
WHO criteria forblastic transformation
Presence of one or more of the following features
● Blast in the peripheral blood or bone marrow more than 20 %
● Blast proliferation at a site other than the bone marrow
● Focal clustering of the blast in bone marrow
Occasionally CML does not follow this pattern, but transform
to myelofibrosis
32.
TREATMENT
The treatment ofhematological malignancy has improved
greatly since the first effective chemotherpeutic drugs were
introduced. This has resulted from developments in both;
● Supportive therapy
● Specific/Definitive therapy
33.
TREATMENT
General/Supportive Therapy
● Adequatehydration
● Blood and blood products as the needs may be
● Tumour lysis syndrome (Allopurinol and Rasburicase)
● Pain management
● Prophylaxis and treatment of infection
● Psychosocial support
34.
TREATMENT
Definitive therapy
● Cytoreductivetherapy;this is achieved with
● Hydroxyurea
● Busulphan
● Cyclophosphamide
● Fludarabine or Cytarabine
Curative therapy
● Imatinib mesylate
● Allogeneic bone marrow transplant
35.
FOLLOW UP
● Regularfollow up
● Monitoring response to therapy
● Assessing treatment failure
● Modifying treatment
36.
MODE OF ACTIONOF
IMATINIB MESYLATE
Mode of action of imatinib mesylate Imatinib mesylate, also
known as Gleevec, is a tyrosine kinase inhibitor (TKI) used to
treat certain types of cancer, including
● CML
● GIST
● MDS
37.
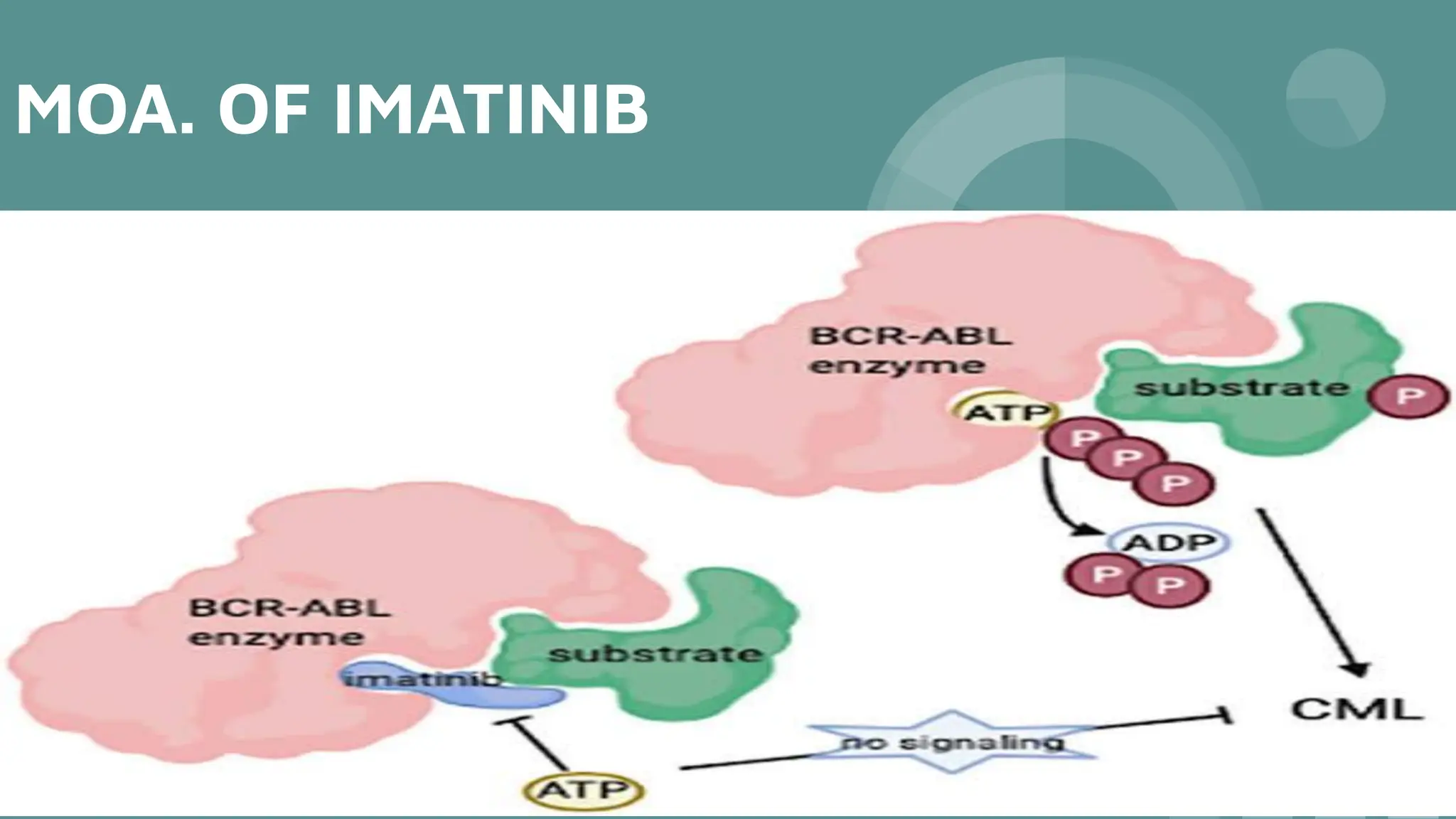
MOA. OF IMATINIB
InCML Imatinib mesylate binds to the ATP-binding site of the
BCR-ABL tyrosine kinase, preventing the transfer of phosphate
groups to signaling molecules. This inhibits the proliferation and
survival of CML cells
CONCLUSION
● Chronic myeloidleukaemia is a clonal disorder of a
pluripotent stem cell. The disease accounts for around
15% of leukaemias and may occur at any age, but is most
common between age 40 and 60 years
● All cases of CML have a translocation between
chromosomes 9 and 22. This leads to generation of the
Philadelphia (Ph) chromosome
● The clinical features include weight loss, sweating,
anaemia, bleeding and splenomegaly
40.
CONCLUSION
● Treatment iswith tyrosine kinase inhibitors such as imatinib,
dasatinib or nilotinib
● Stem cell transplantation can be curative and may also be
useful for advanced disease
● The clinical outcome is now very good and 90% of patients
can expect long‐term control of disease
41.
REFERENCE
● Hoffbrand EssentialHaematology 8th. Edition
● Shirish M. Kawthalkar Essential of Haematology
● htpp/Medscape.org
CLINICAL SCENARIO
A 32year old Disco Jockey presented at the
oto-rhino-laryngology unit with sudden hearing loss in both ears.
Laboratory investigation revealed marked neutrophilic
leucocytosis, for which he was referred for haematological
review. Patient also gave a history of progressive malaise in the
last six months, with associated weight loss, night sweats and
progressive left sided abdominal fullness. Significant examination
findings were those of wide spread bean size nodular swellings
in the upper and lower extremities, and splenomegaly of 24 cm
below the left costal margin.
FOLLOW UP QUESTIONS
●What is the most likely diagnosis?
● What other history will you be interested in?
● Enumerate on the clinical findings
● Interpret the FBC result and expected peripheral blood
examination findings
● What other investigations will you do?
● How will you treat this patient?
● What is the role of Hydroxyurea in this patient
● Discuss complications of CML


































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)













