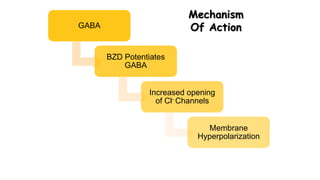
Clinical toxicology deals with diseases caused by toxic substances. The initial clinical approach to a poisoned patient involves stabilization, evaluation through history, physical exam and tests, prevention of further toxin absorption, enhancement of elimination, administration of antidotes, and supportive care. Prevention methods include removal from environment, washing skin, and gastric lavage. Enhancement methods include alkalinization of urine, hemodialysis, and activated charcoal. Barbiturates and benzodiazepines are central nervous system depressant drugs that can induce sleep or calmness without sleep, and toxicity from overdose requires supportive care and flumazenil or physostigmine as antidotes.