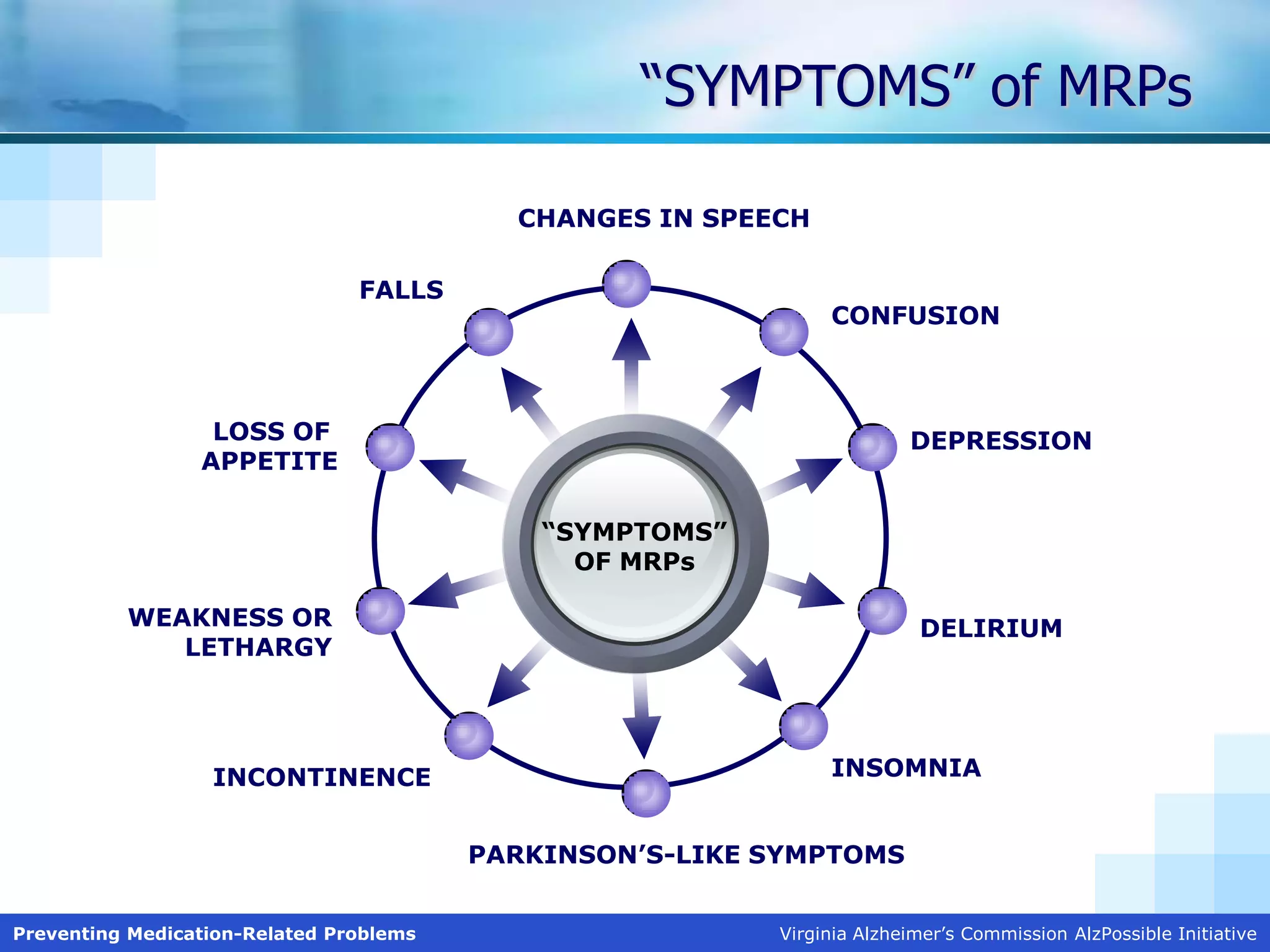
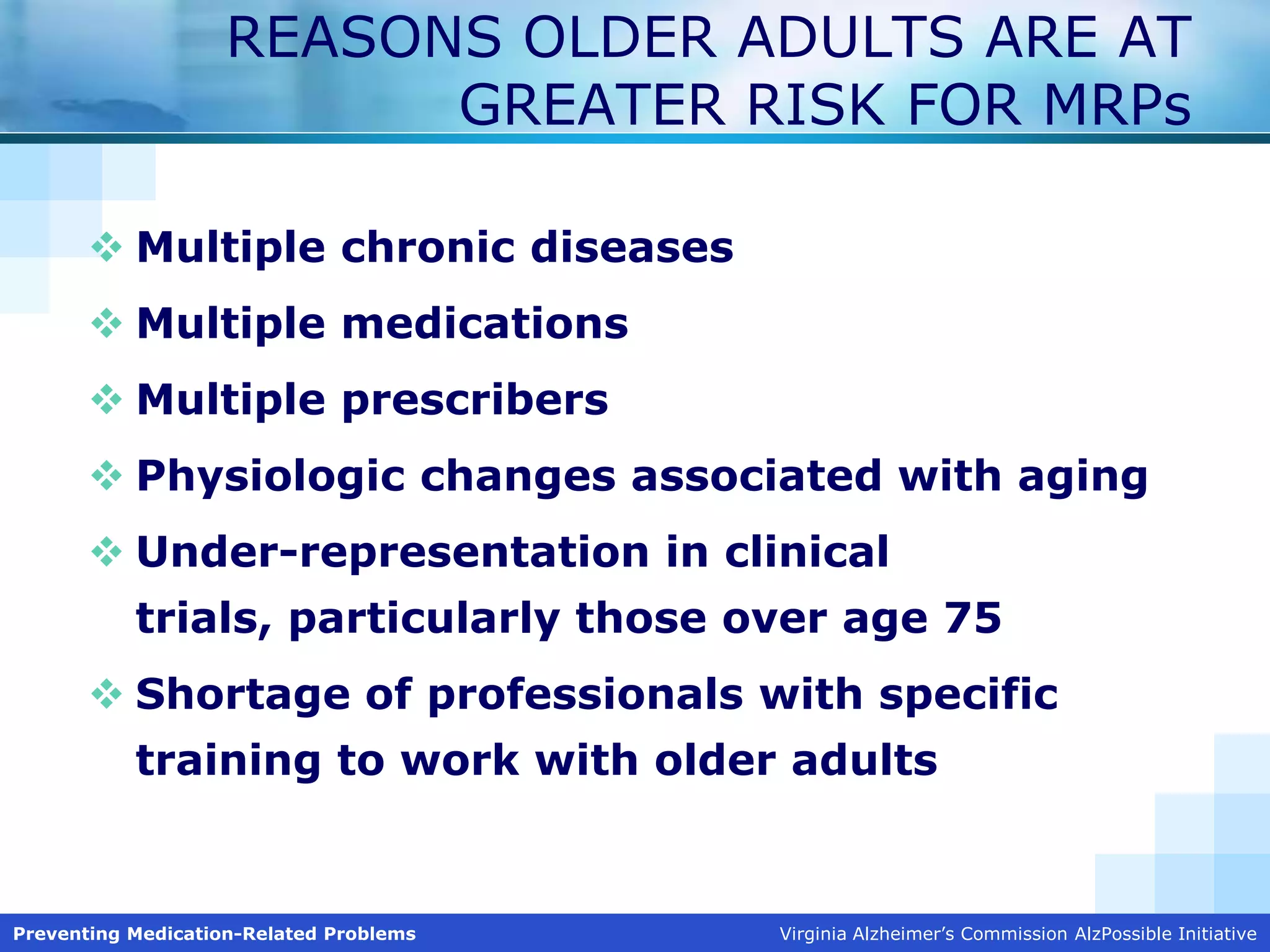
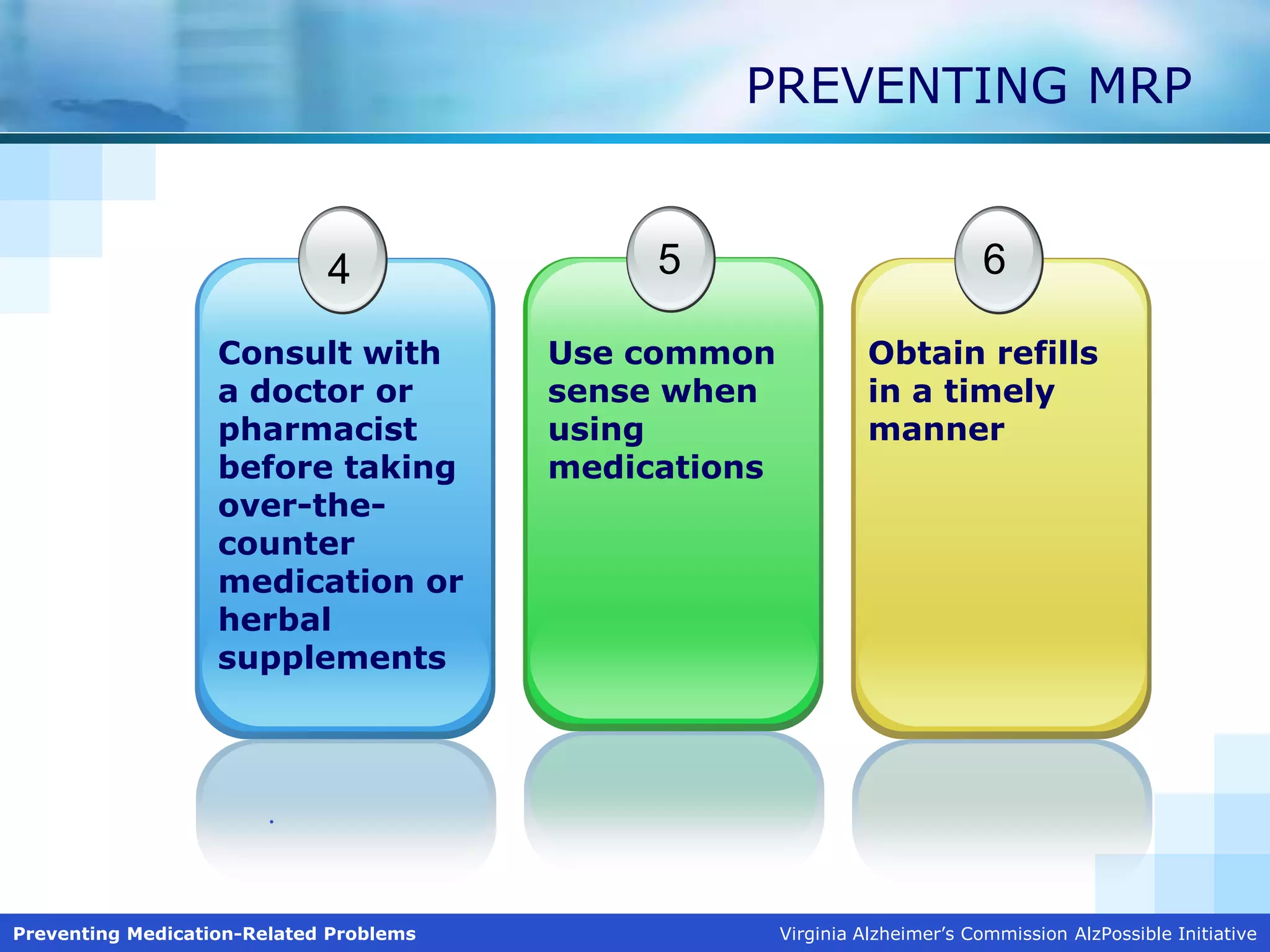
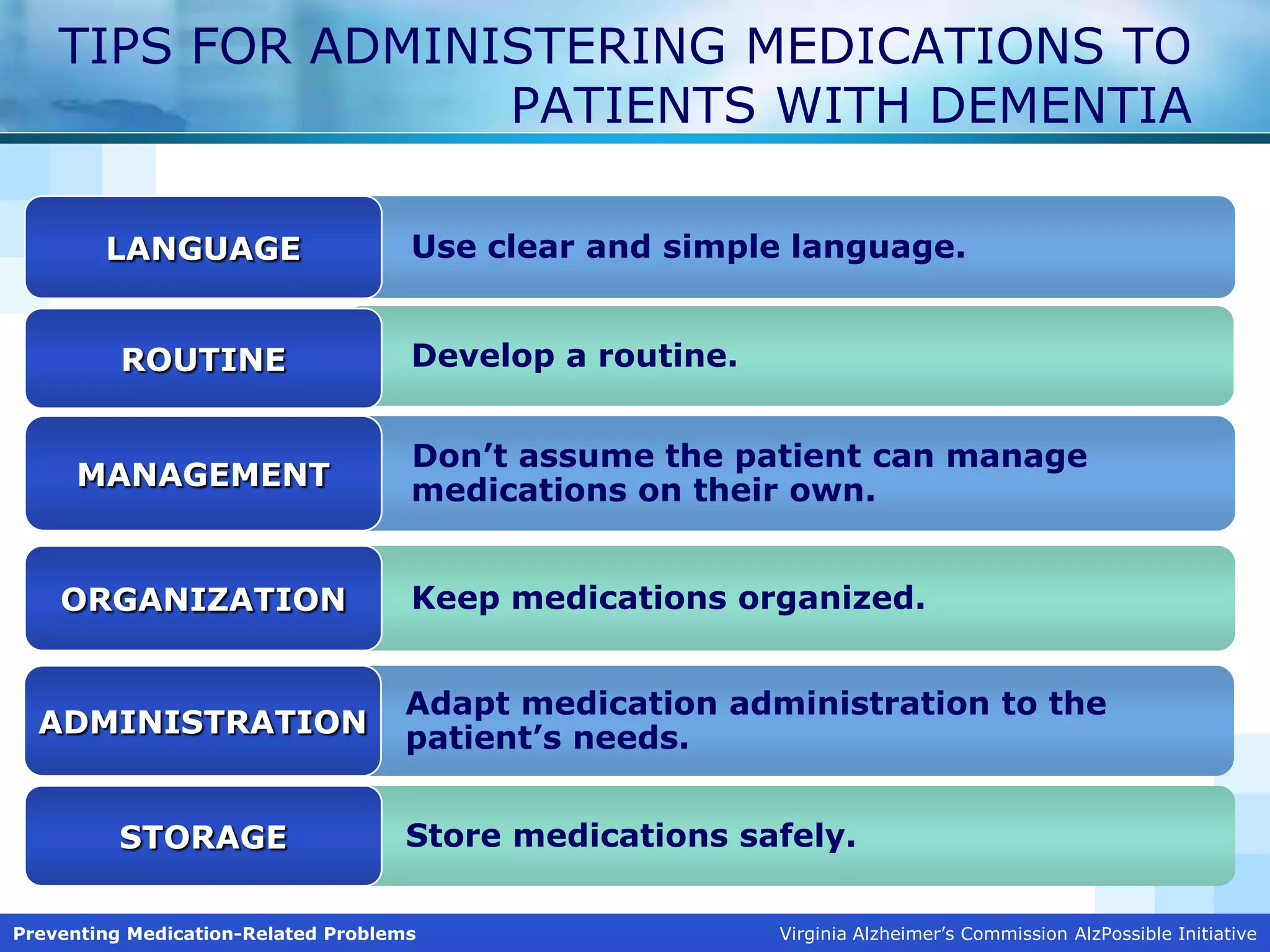
Medications are an important tool for preventing illness and disability in older populations, but they can also cause medication-related problems (MRPs). MRPs are undesirable events involving drug therapy that interfere with patient outcomes. Common symptoms of MRPs include changes in speech, falls, confusion, loss of appetite, weakness, incontinence, insomnia, and Parkinson's-like symptoms. Older adults are more at risk for MRPs due to multiple chronic diseases, medications, prescribers, and age-related physiological changes. The presentation provides tips for preventing MRPs such as designating a medication manager, keeping an accurate medication list, consulting providers before starting new medications, and developing routines for administering medications to patients





























































![Geriatric Syndromes [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/geriatricsyndromesautosaved-230726141128-89b23bf0-thumbnail.jpg?width=640&height=640&fit=bounds)



























