Download to read offline

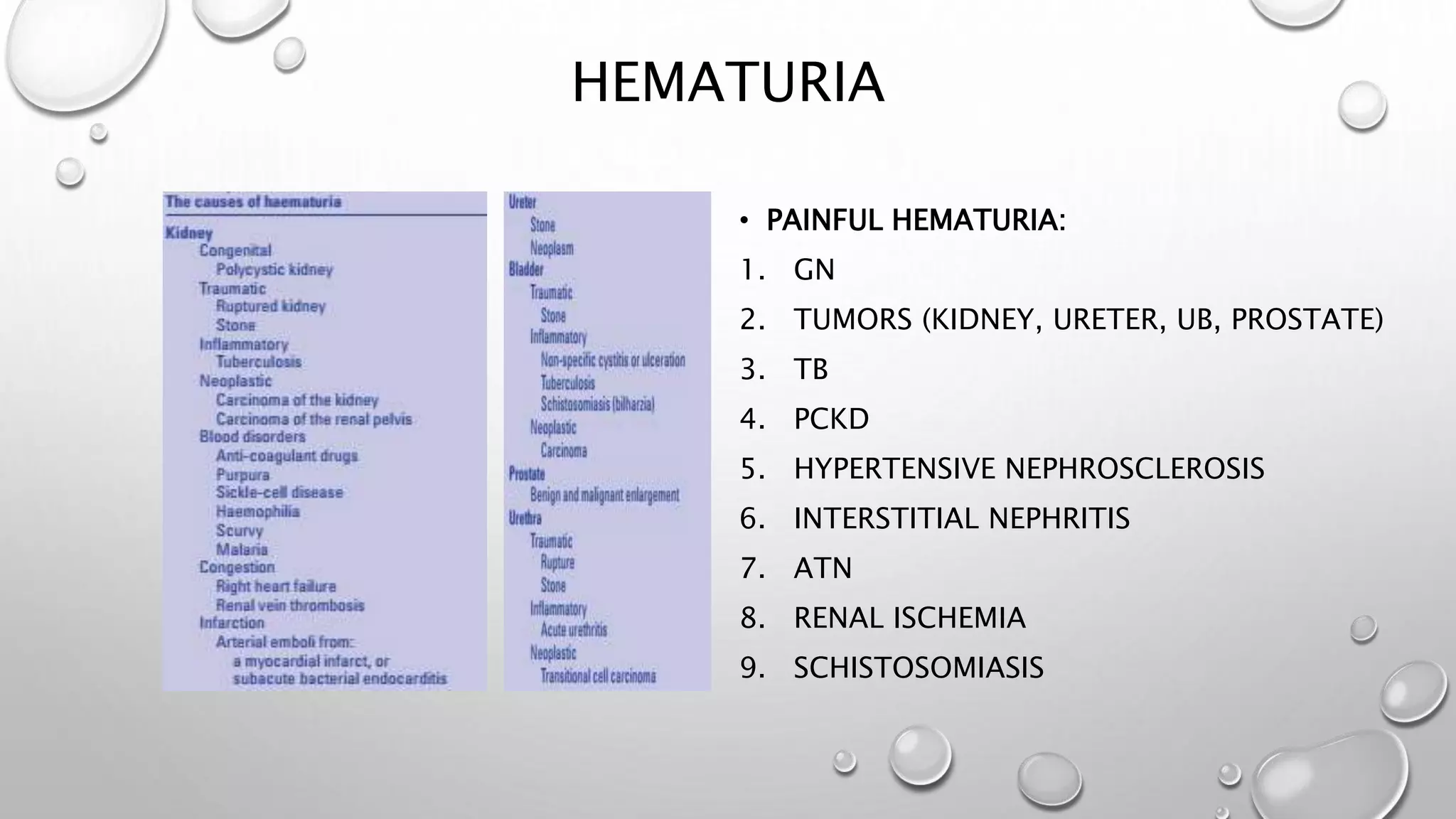




This document discusses the clinical presentation of urological patients through symptoms and signs. It covers systemic manifestations like fever and weight loss. It also describes local and referred pains associated with different parts of the urinary system like the kidney, ureter, bladder, prostate and testes. Other symptoms discussed include hematuria, pneumaturia, hematospermia and lower urinary tract symptoms. Examination findings of external genitalia are also outlined.







































![Emergency in Urology [Dr. Edmond Wong]](https://cdn.slidesharecdn.com/ss_thumbnails/emergencyuroedmond-140716213857-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)



































