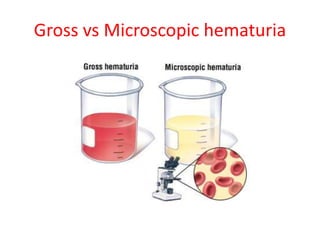
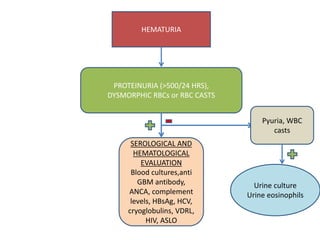
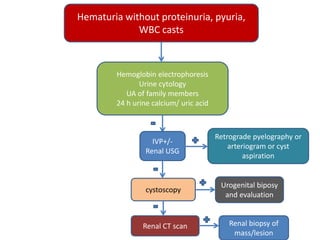
This document provides an approach to evaluating hematuria, or blood in the urine. It defines hematuria and discusses distinguishing it from pigmenturia or hemoglobinuria/myoglobinuria. Significant hematuria is described as more than 3 red blood cells per high power field on 3 urine analyses or a single analysis with over 100 red blood cells or gross hematuria. A history and physical exam can provide clues to the source and causes of hematuria. Additional testing includes urine analysis, blood tests, imaging and potentially renal biopsy. Common causes include stones, tumors, infections, bleeding disorders and glomerulonephritis. An algorithm is provided outlining evaluation and management based on urine findings.