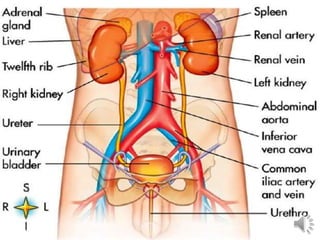
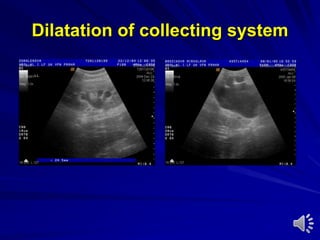
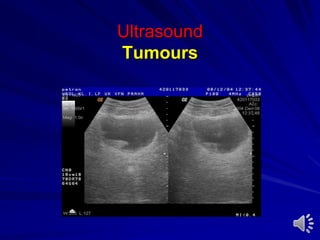
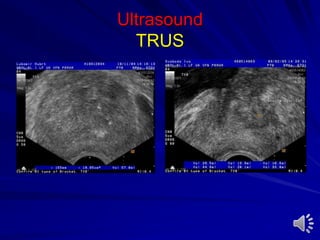
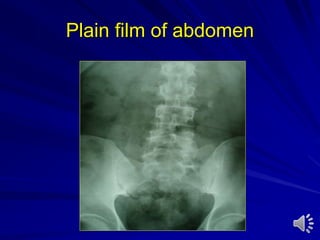
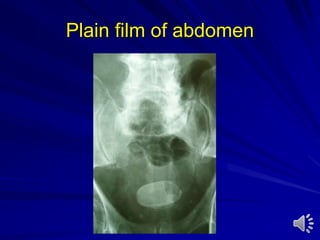
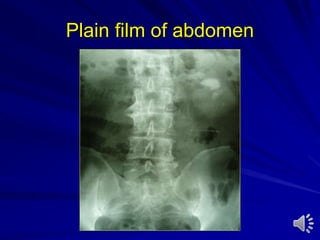
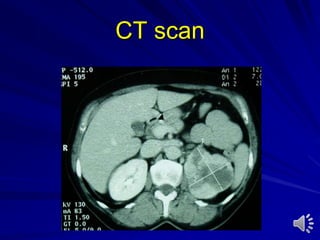
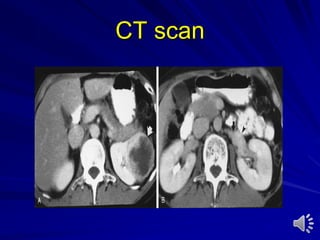
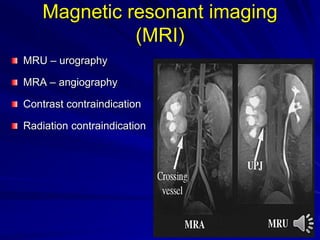
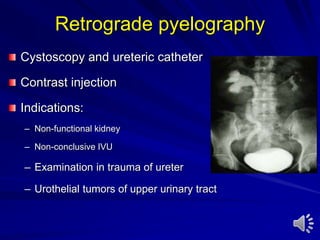
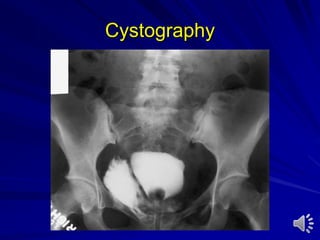
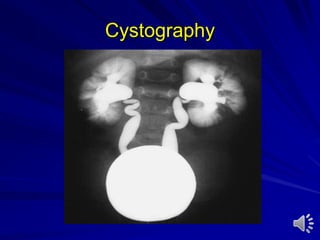
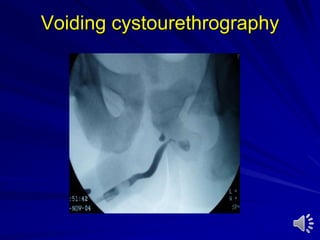
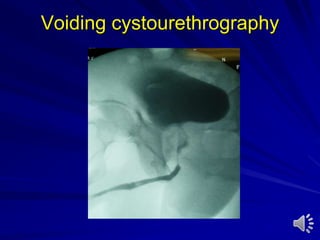
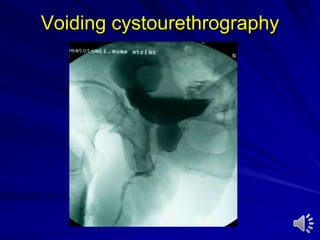
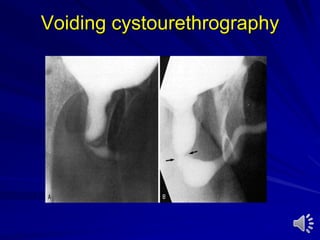
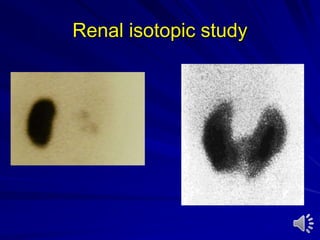
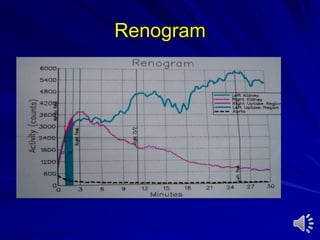
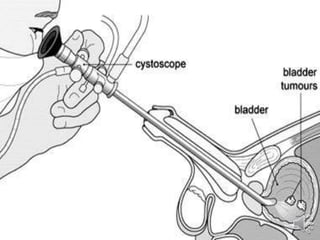
This document provides an introduction and overview of the field of urology. It discusses that urology is the surgical specialty focused on disorders of the genitourinary tract. It also outlines some key points about urology, including that 15% of patients seen by physicians have a urologic complaint, urologists treat patients of all ages and both genders, and the organs and systems within the scope of urology. The document then discusses common urologic symptoms, examinations, investigations including various imaging studies and endoscopic procedures, and diagnostic tests used in urology evaluations and diagnoses.