Downloaded 1,897 times
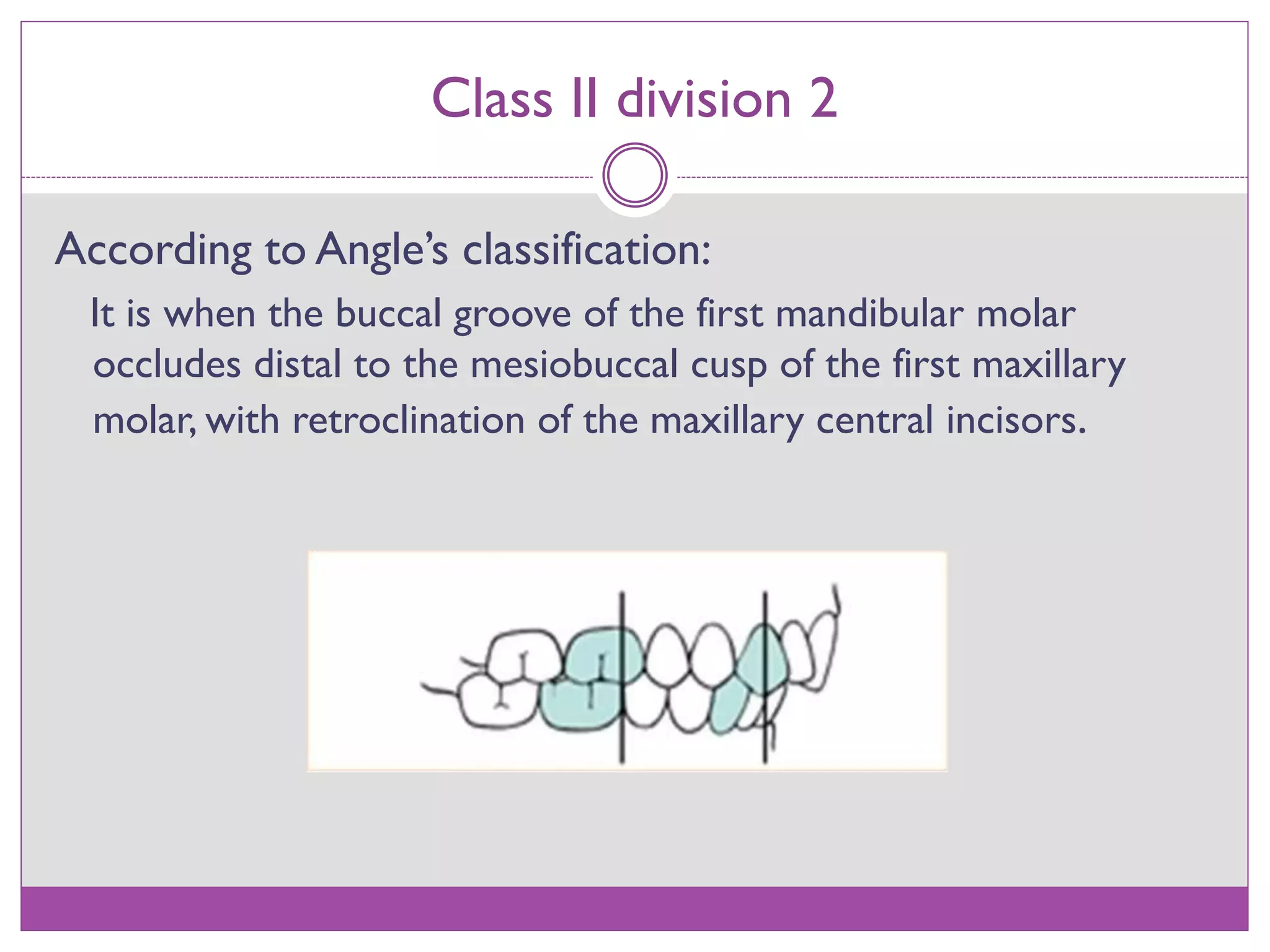
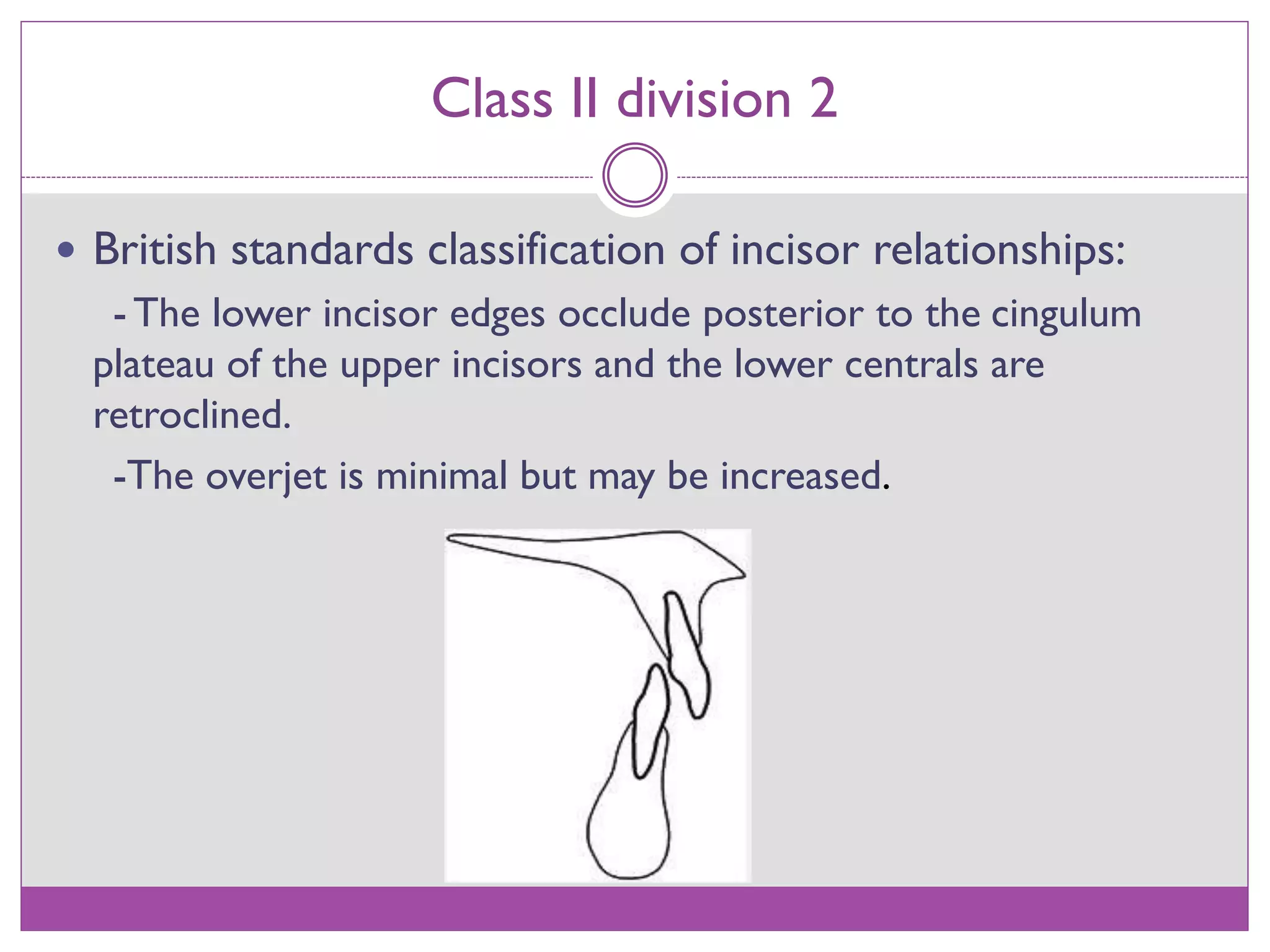
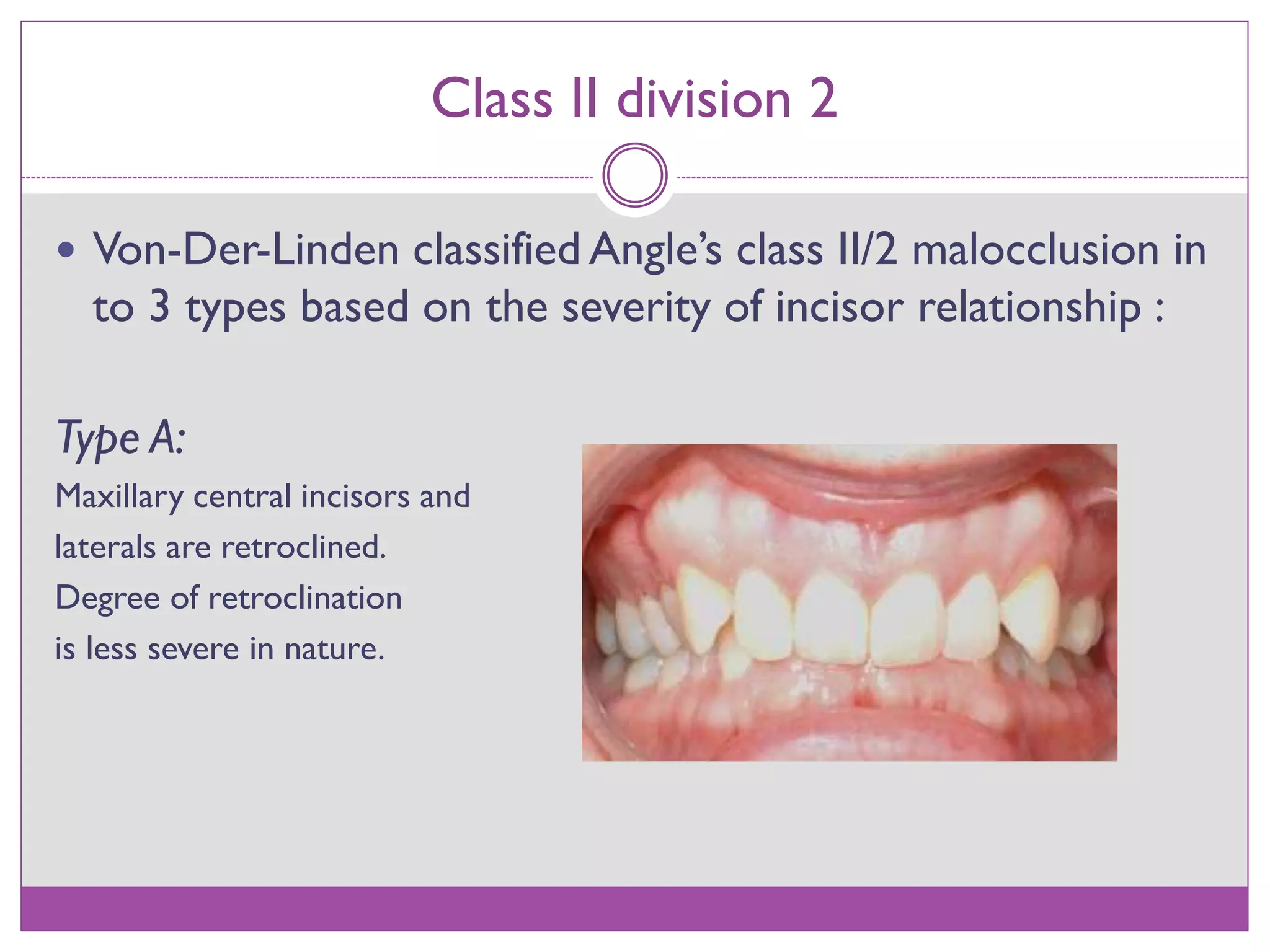

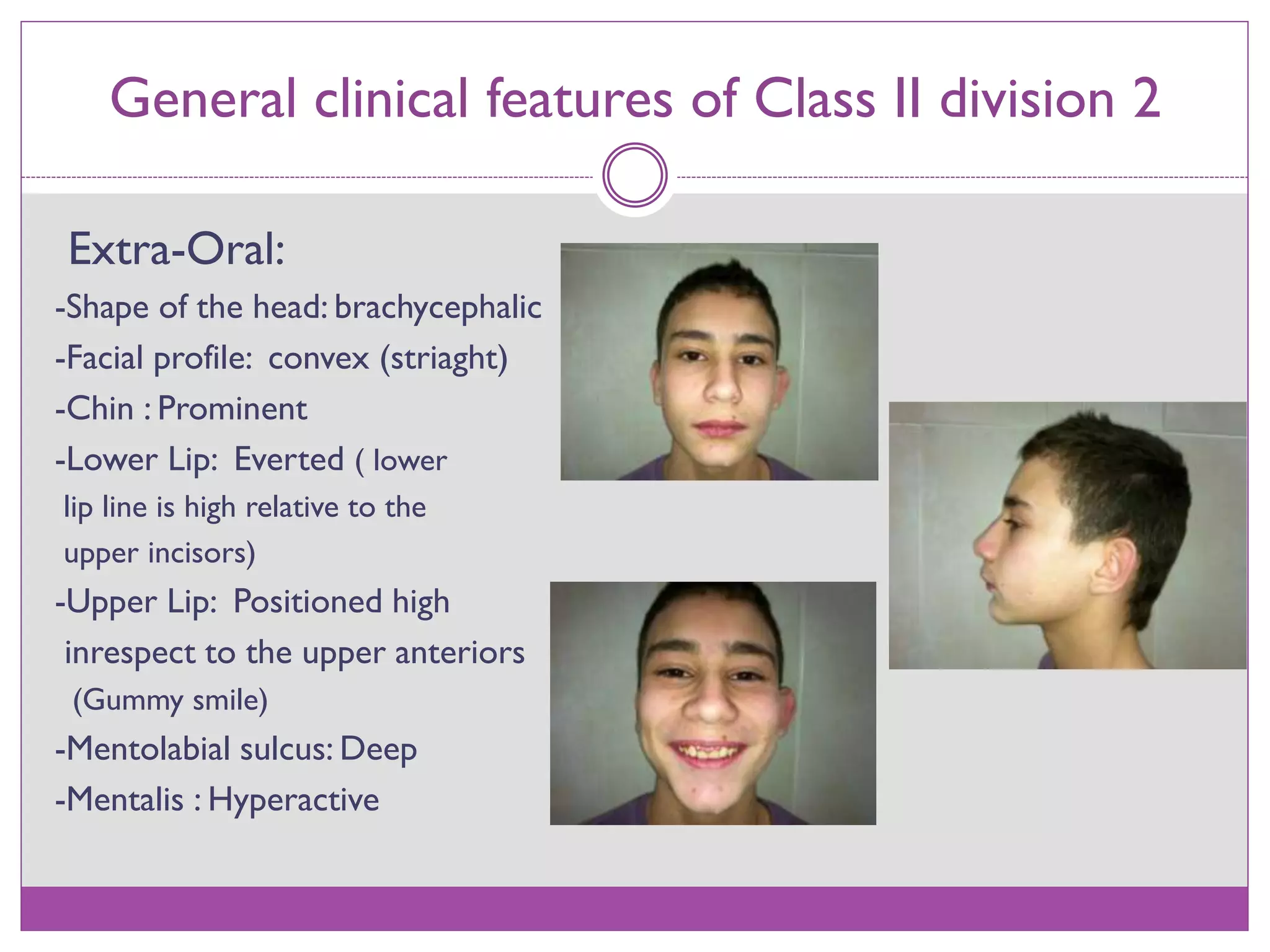
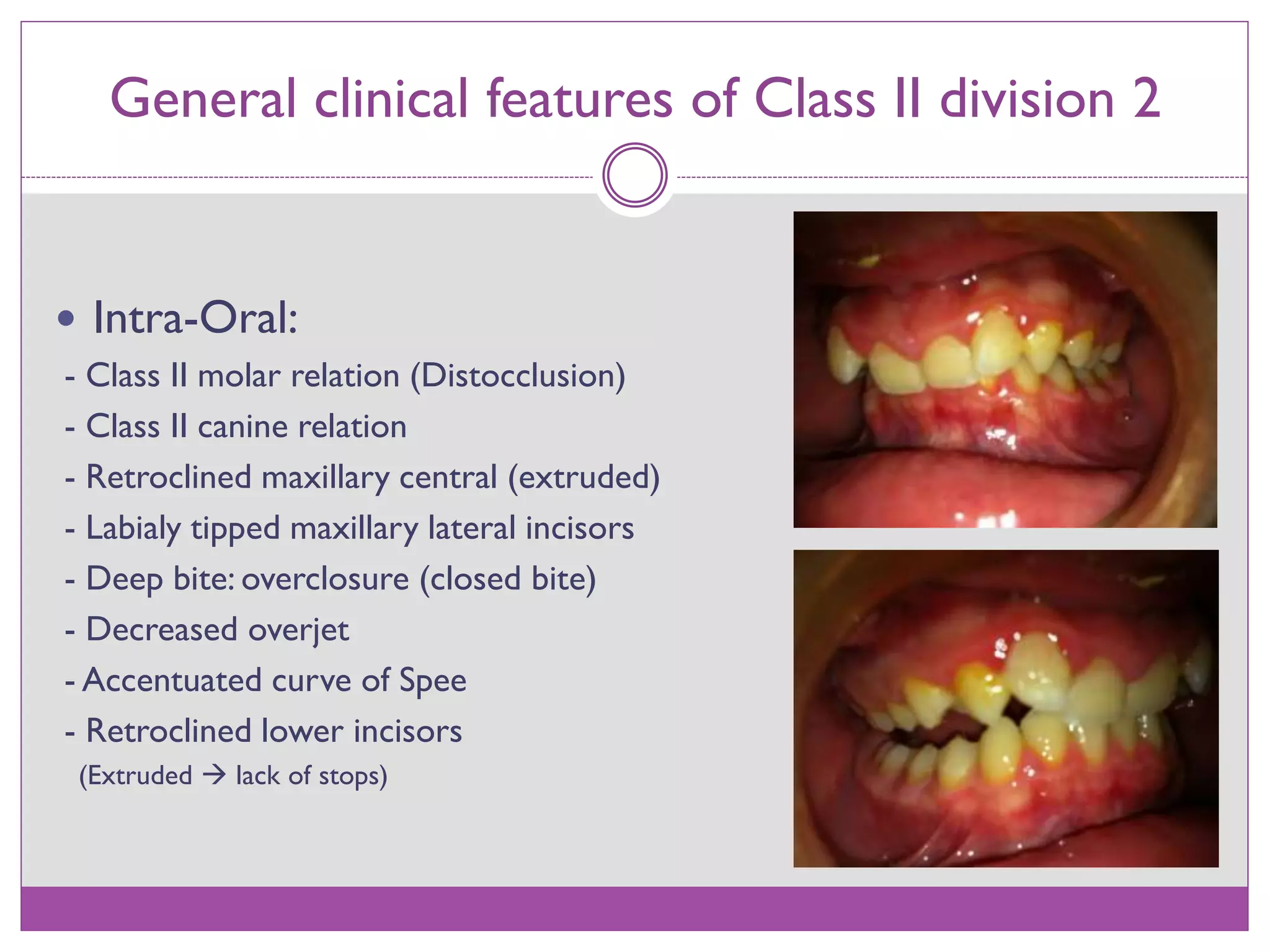
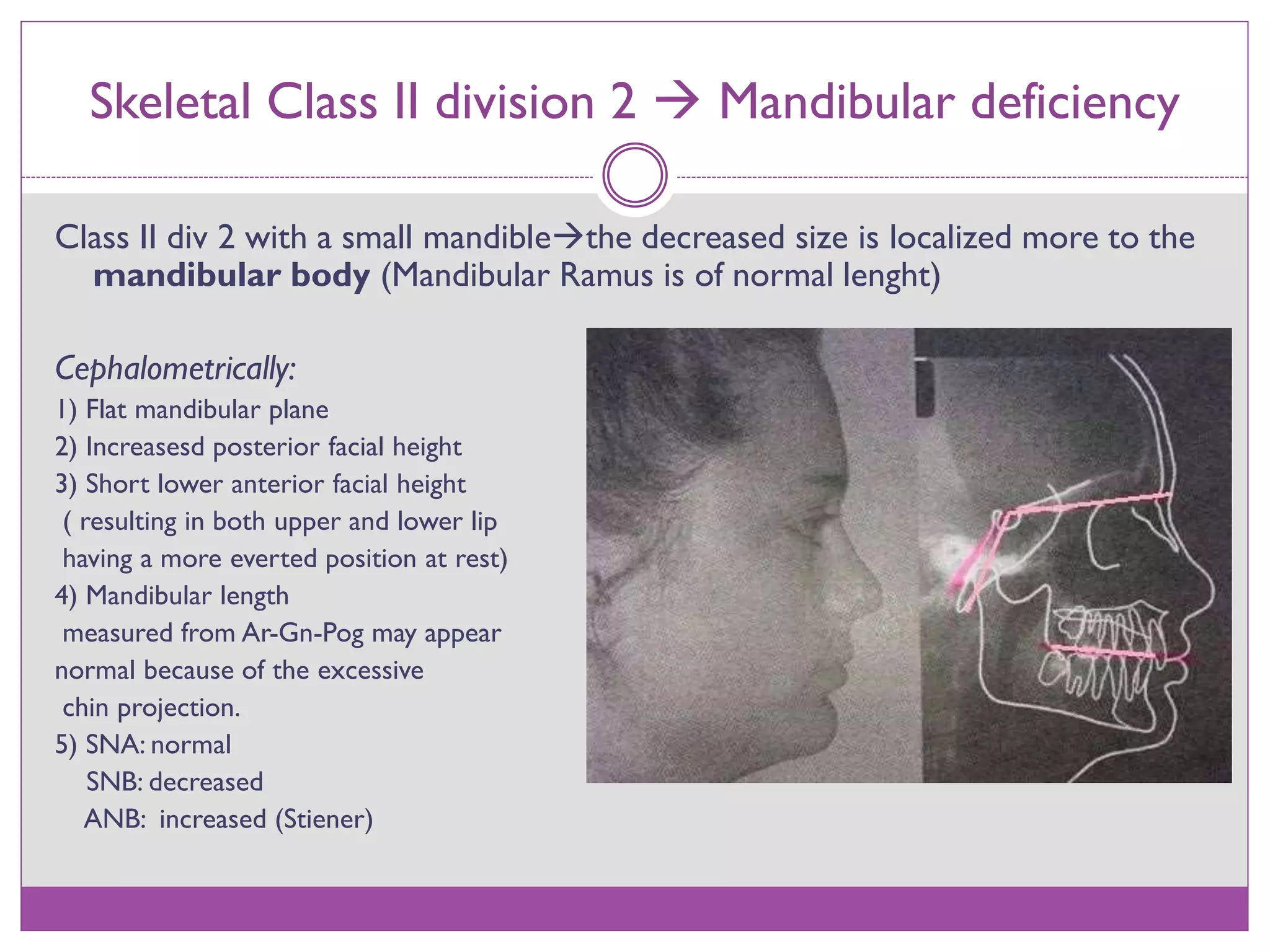
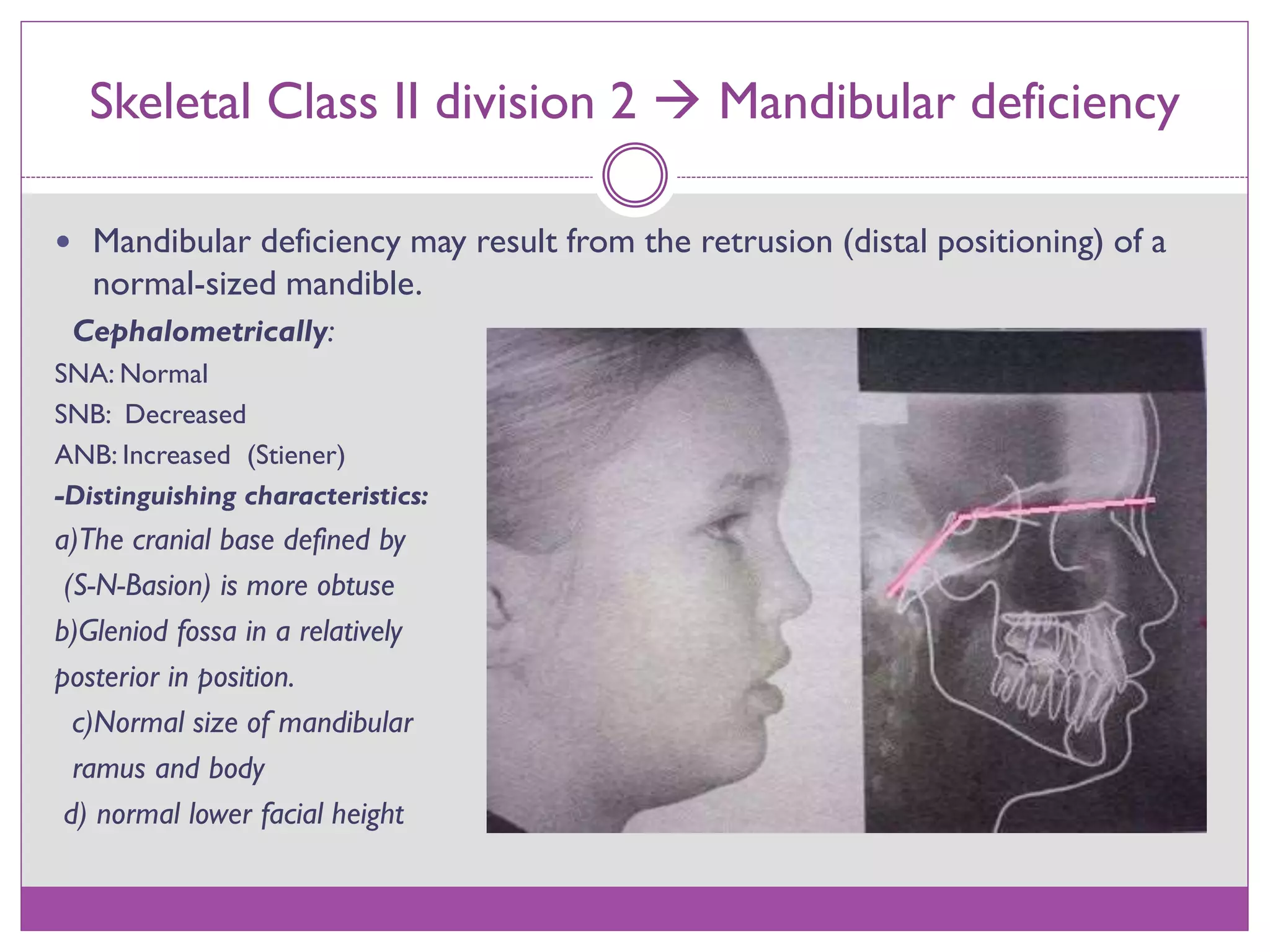
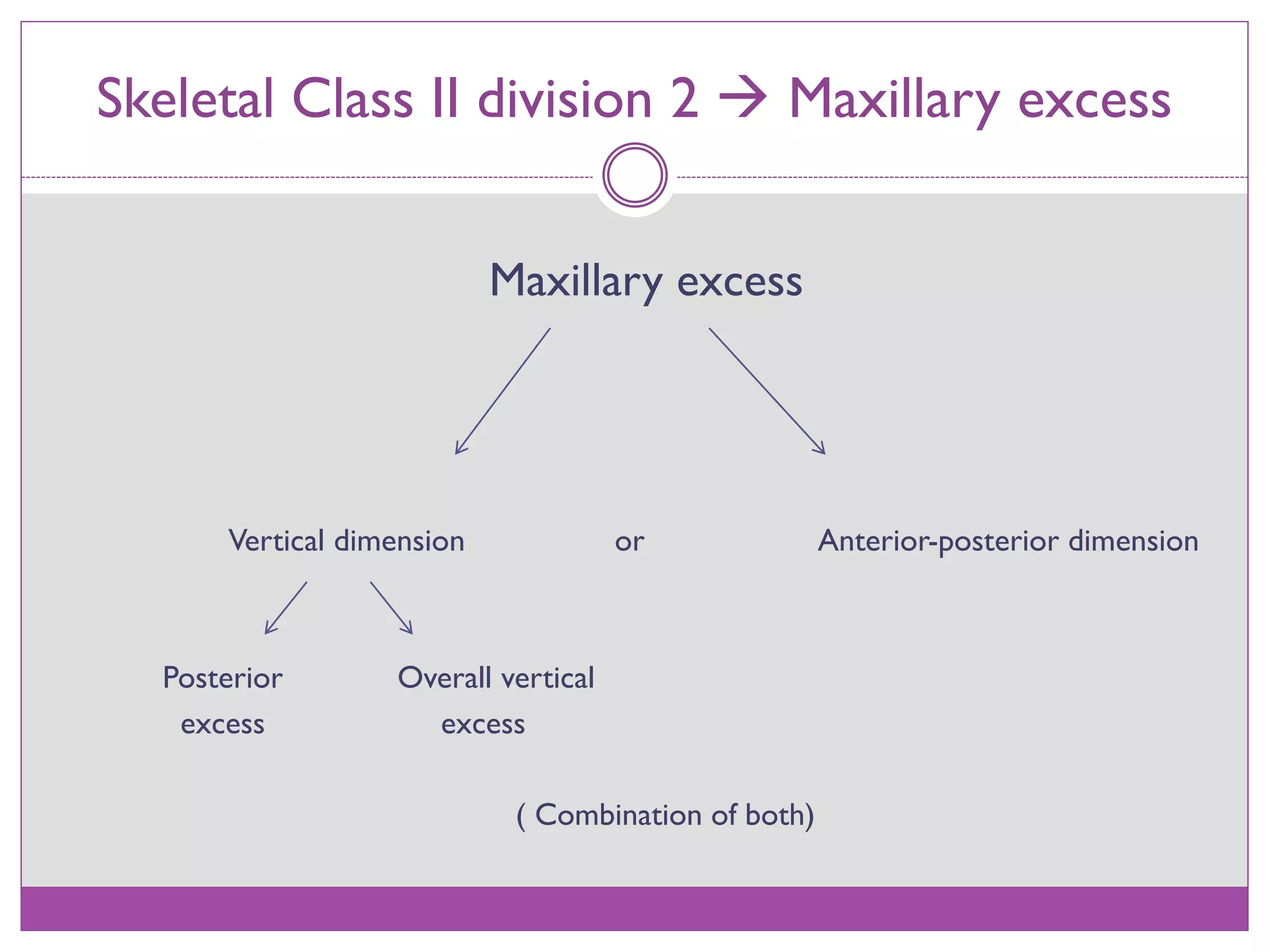
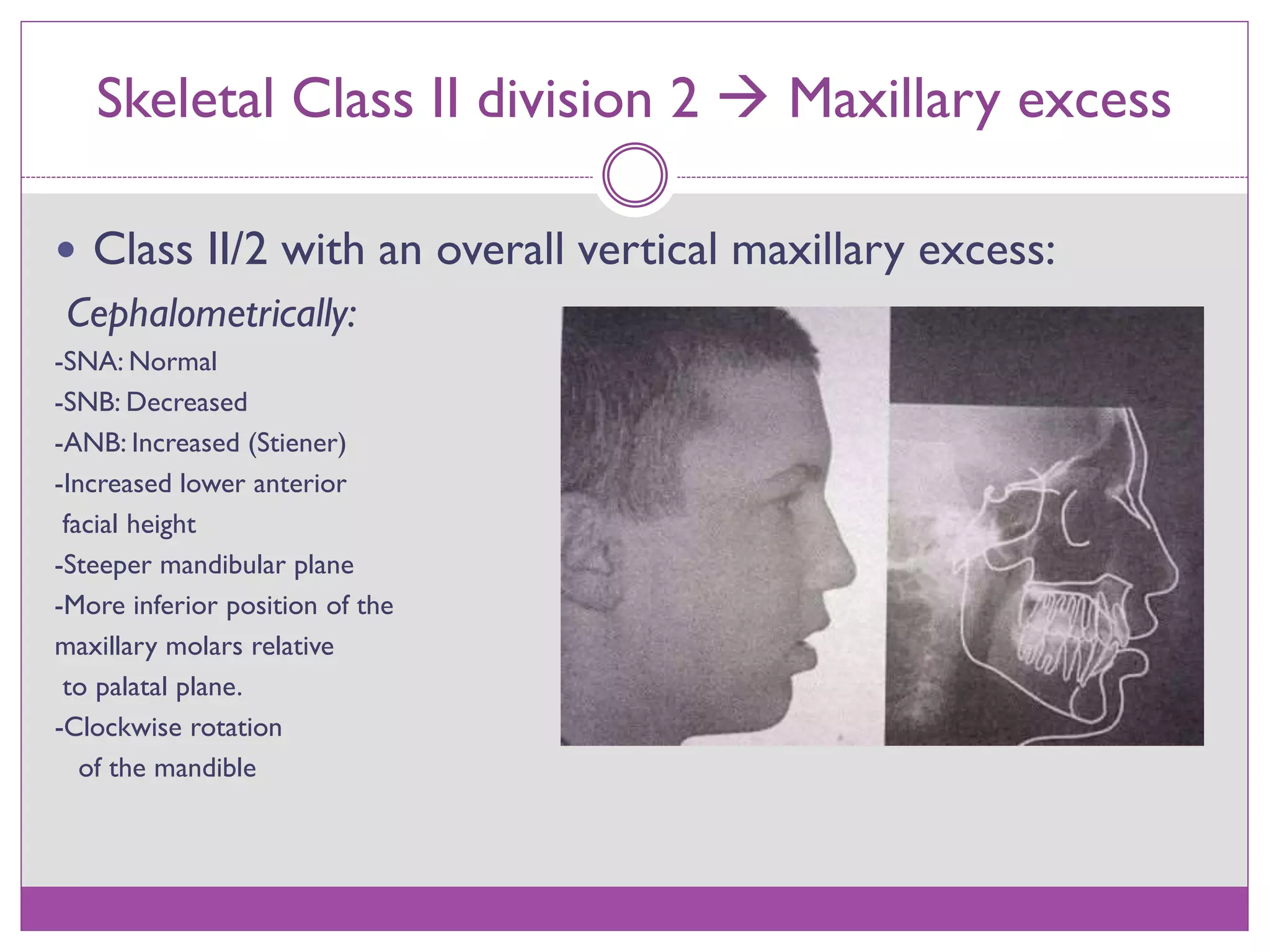
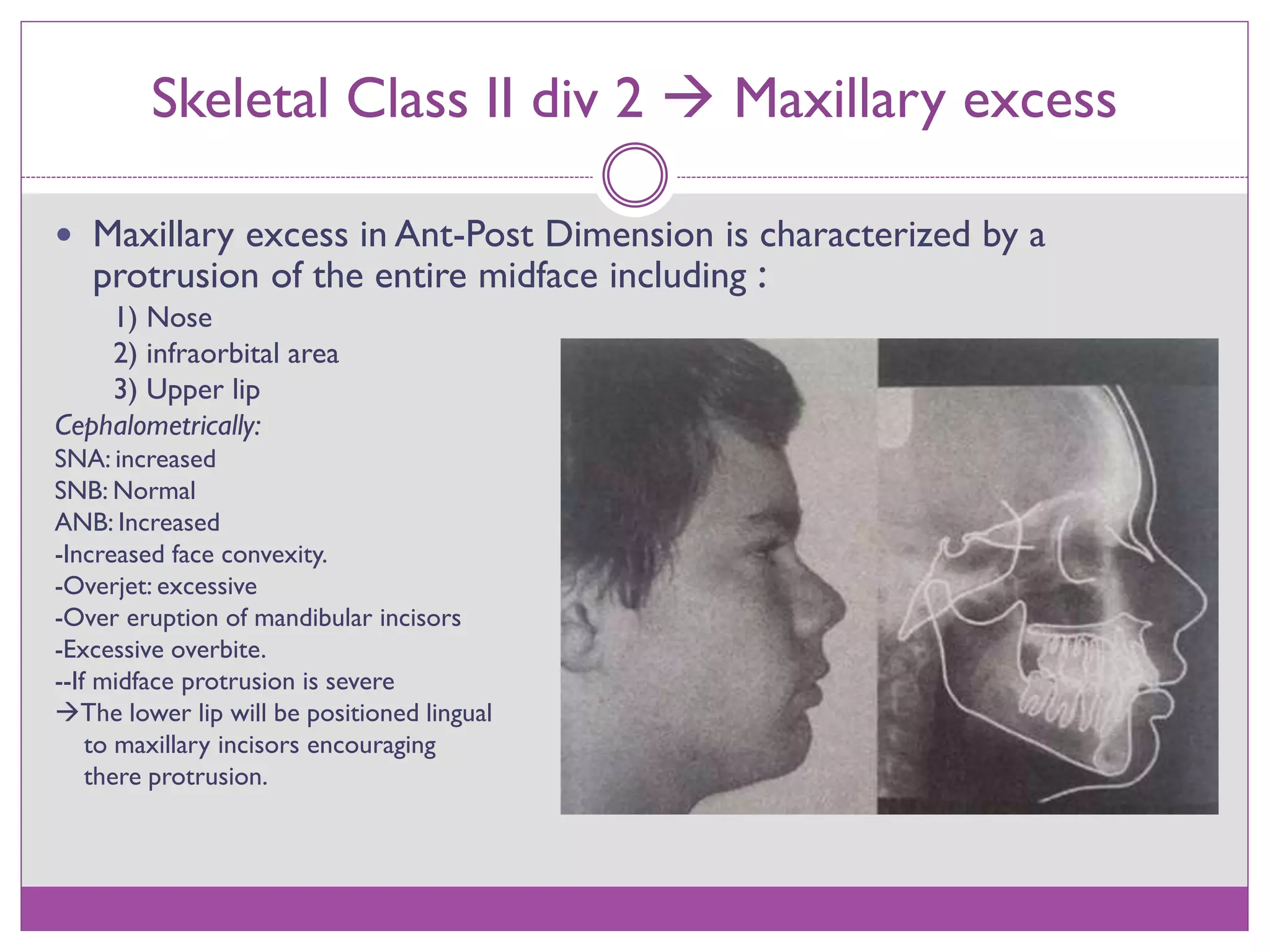
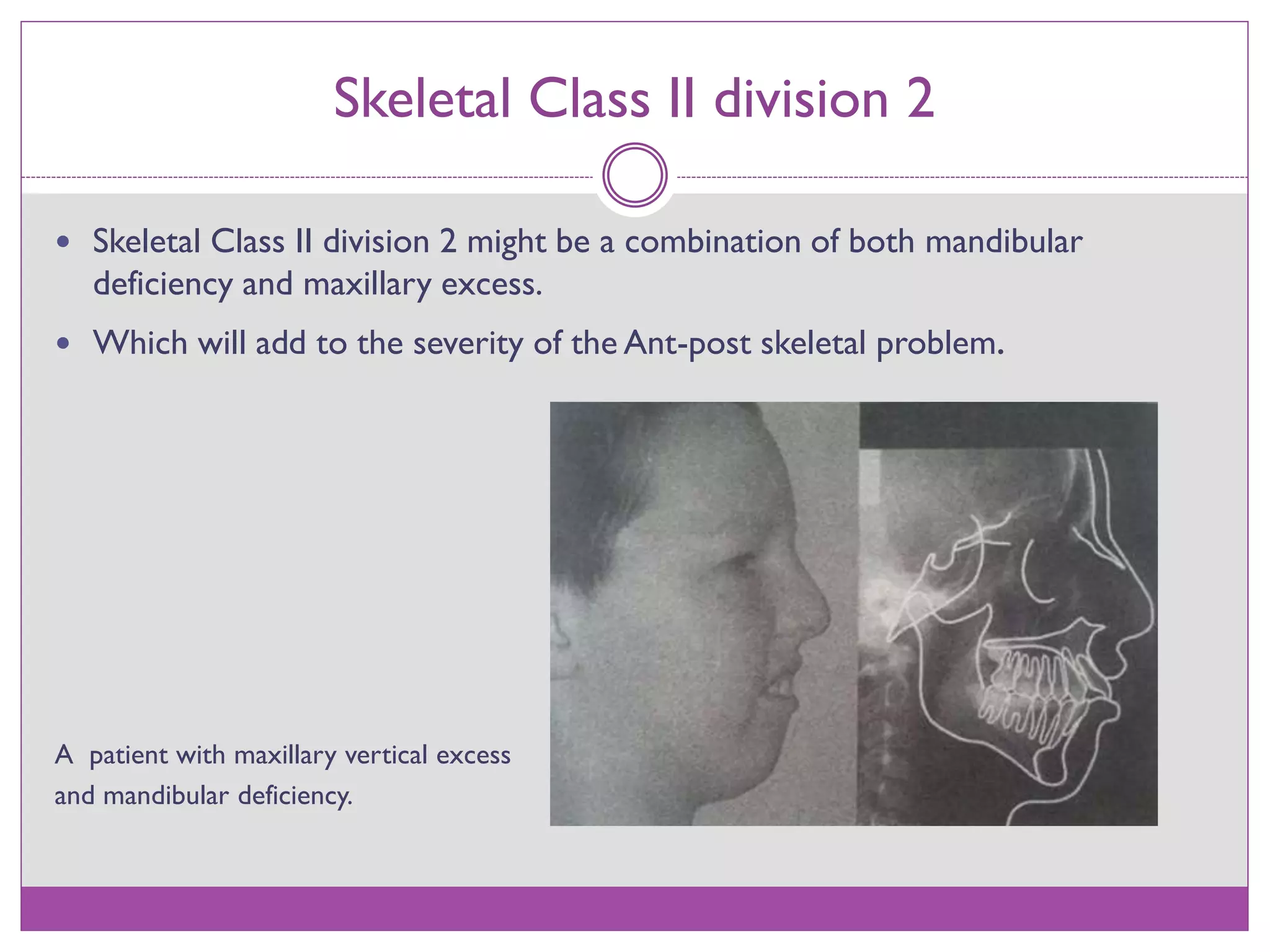
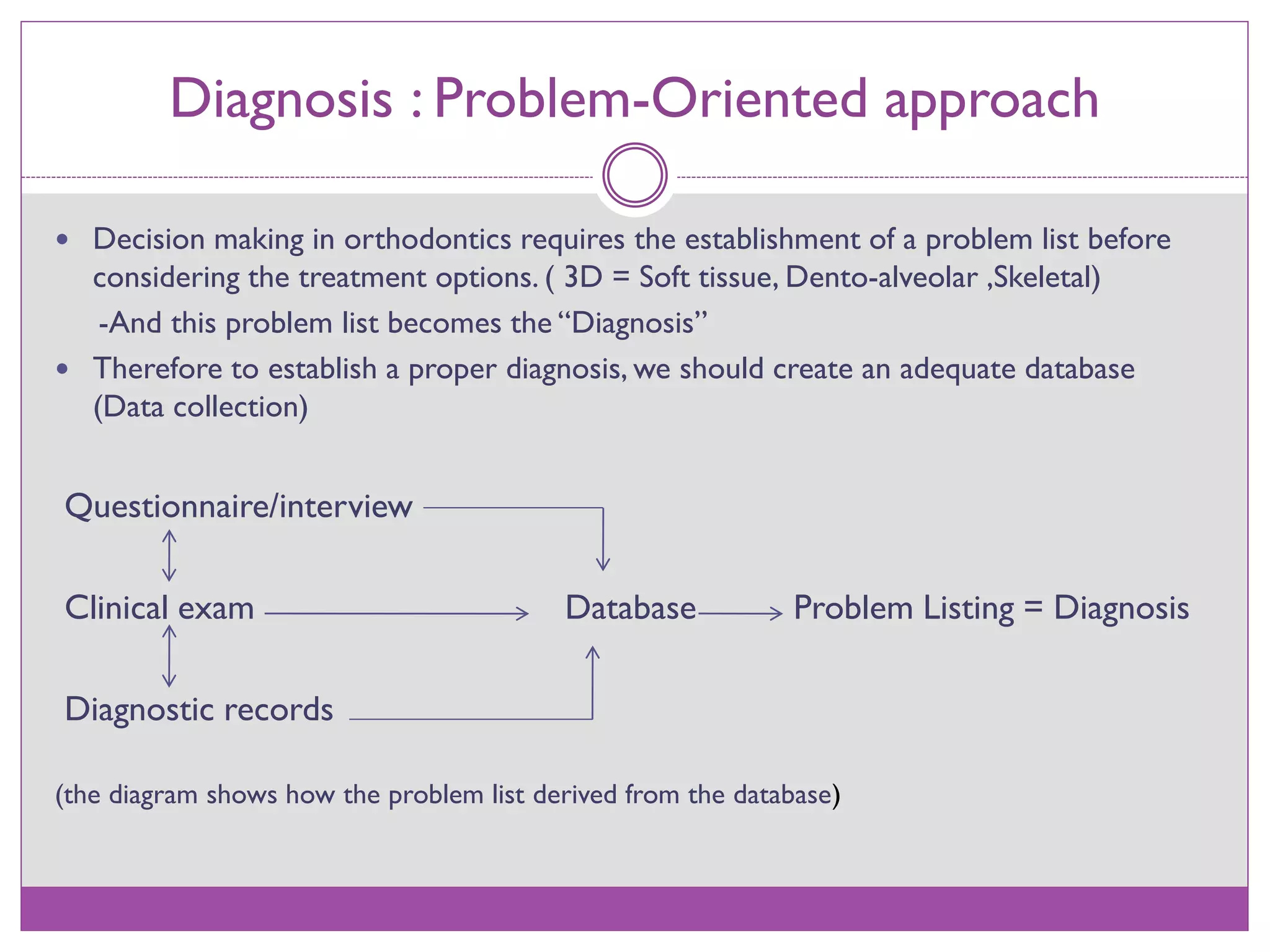









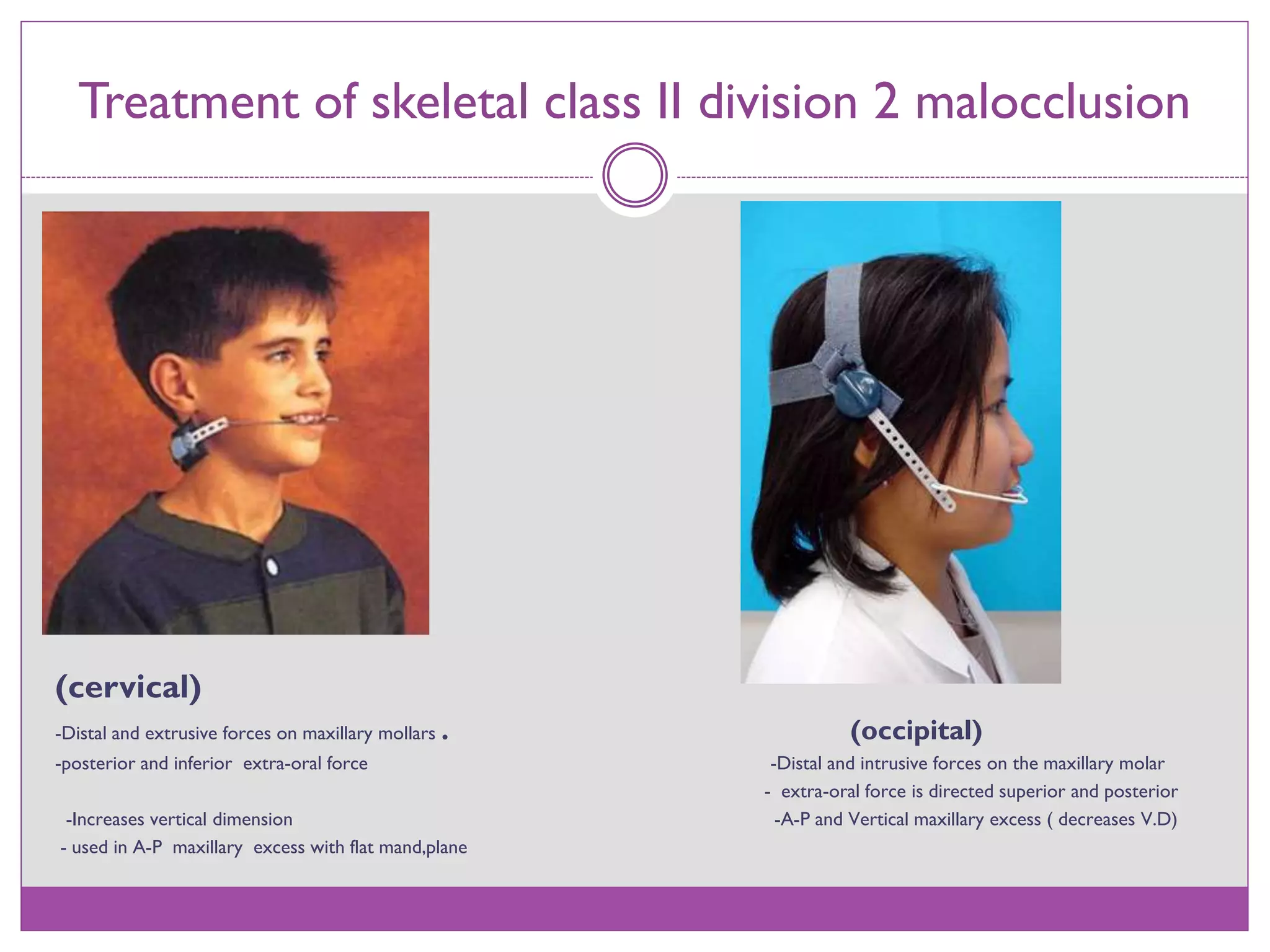
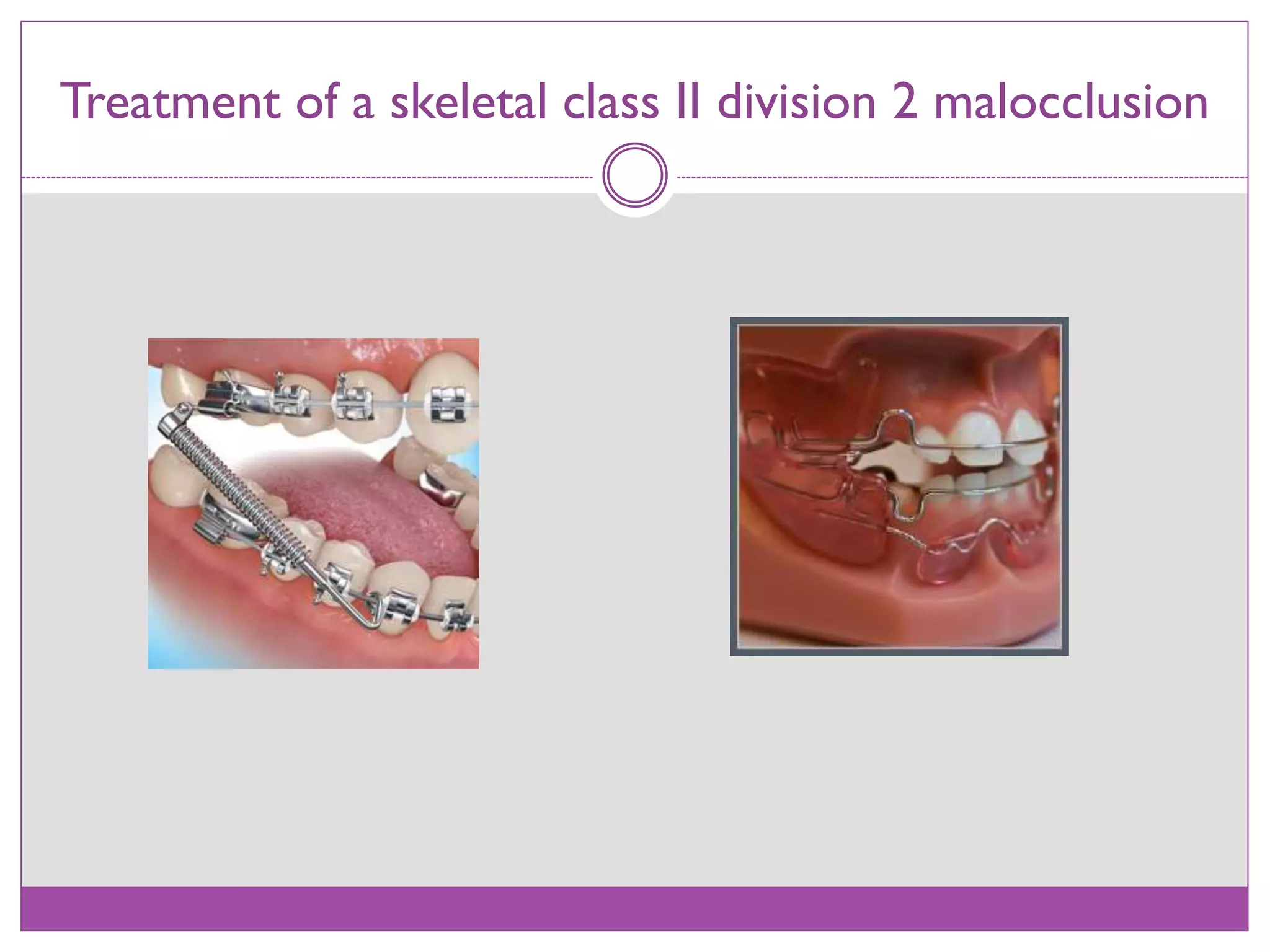




This document discusses Class II division 2 malocclusion, including its definition, classification, clinical features, etiology, diagnosis, and treatment options. Class II division 2 is a type of Class II malocclusion characterized by retroclined maxillary incisors. It can be caused by skeletal factors like mandibular deficiency or maxillary excess, or dental factors like premature tooth loss. Diagnosis involves a problem-oriented approach through data collection and establishing a problem list. Treatment may involve orthodontics alone for mild cases, but more severe cases may require orthodontics combined with orthopedics/growth modification or orthognathic surgery.




















































































