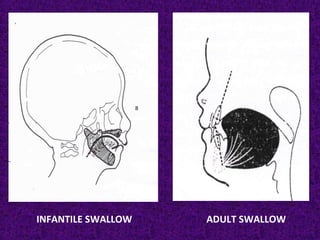
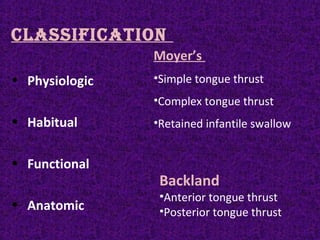
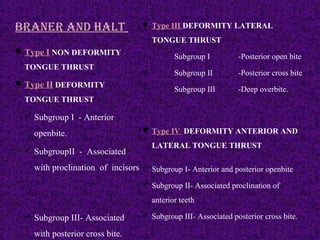
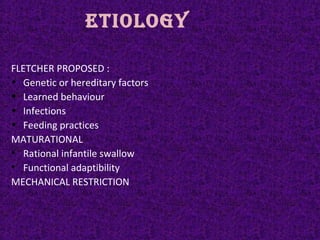
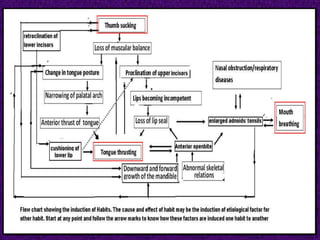
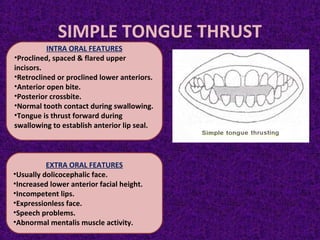
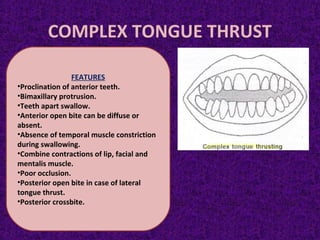
The document explores tongue thrusting, outlining its definitions, classifications, etiology, and management strategies. It discusses the impacts of incorrect swallowing patterns and features of various types of tongue thrusts, including physiological and habitual classifications. Treatment plans involve myofunctional exercises, appliance use, and diagnostic procedures to address oral habits, emphasizing the importance of behavior modification and muscle training.























































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)










![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)





