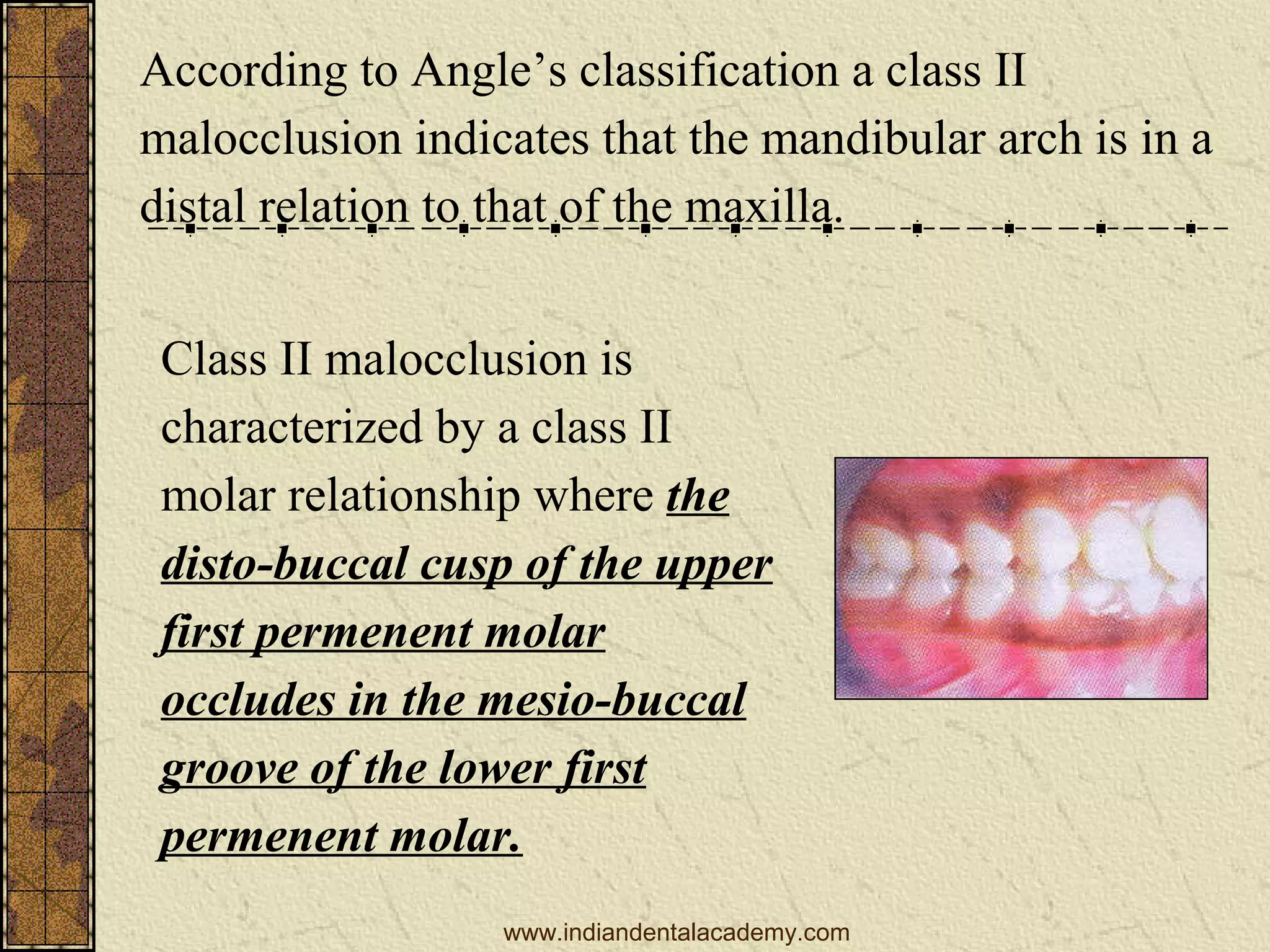
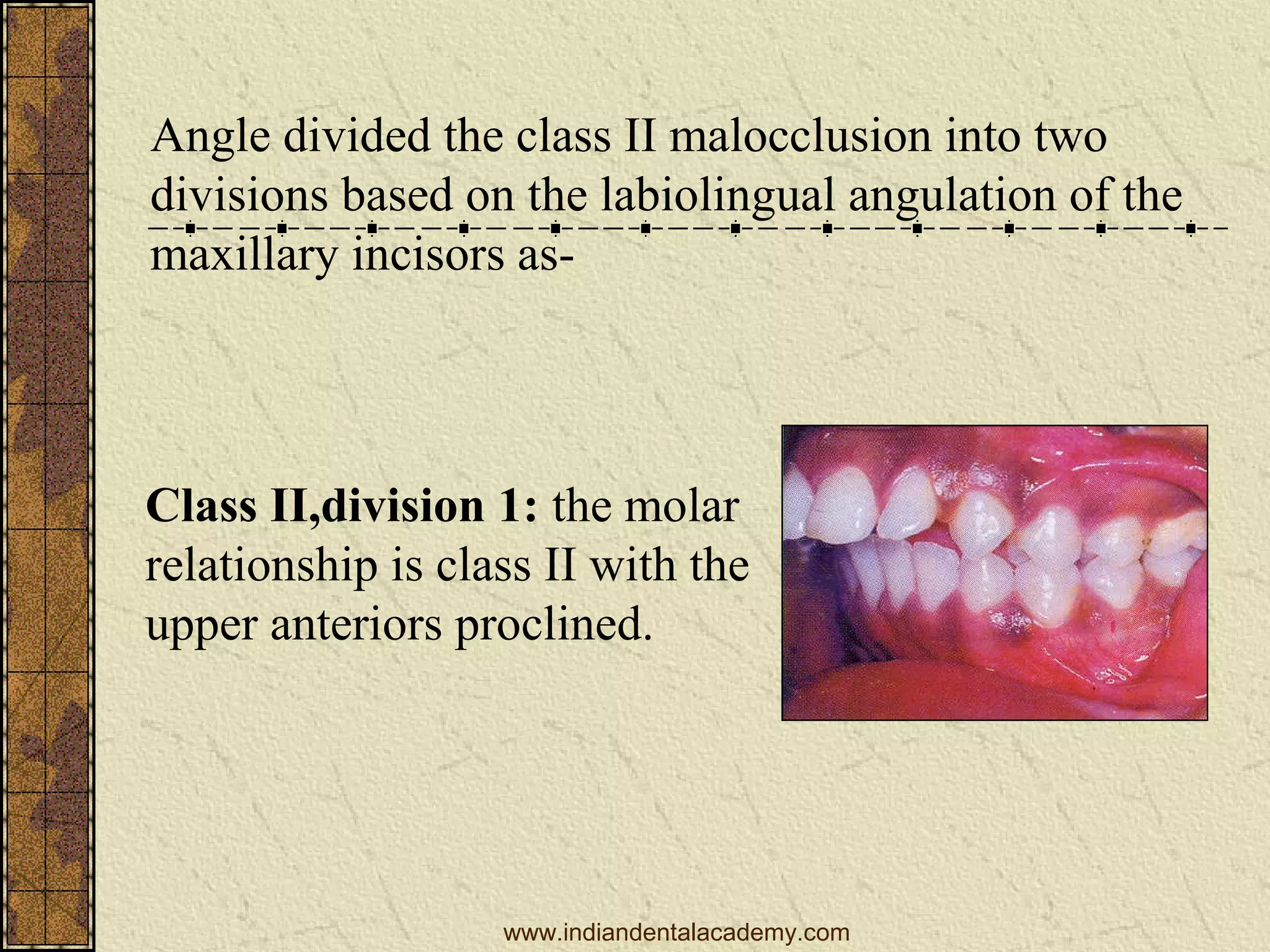
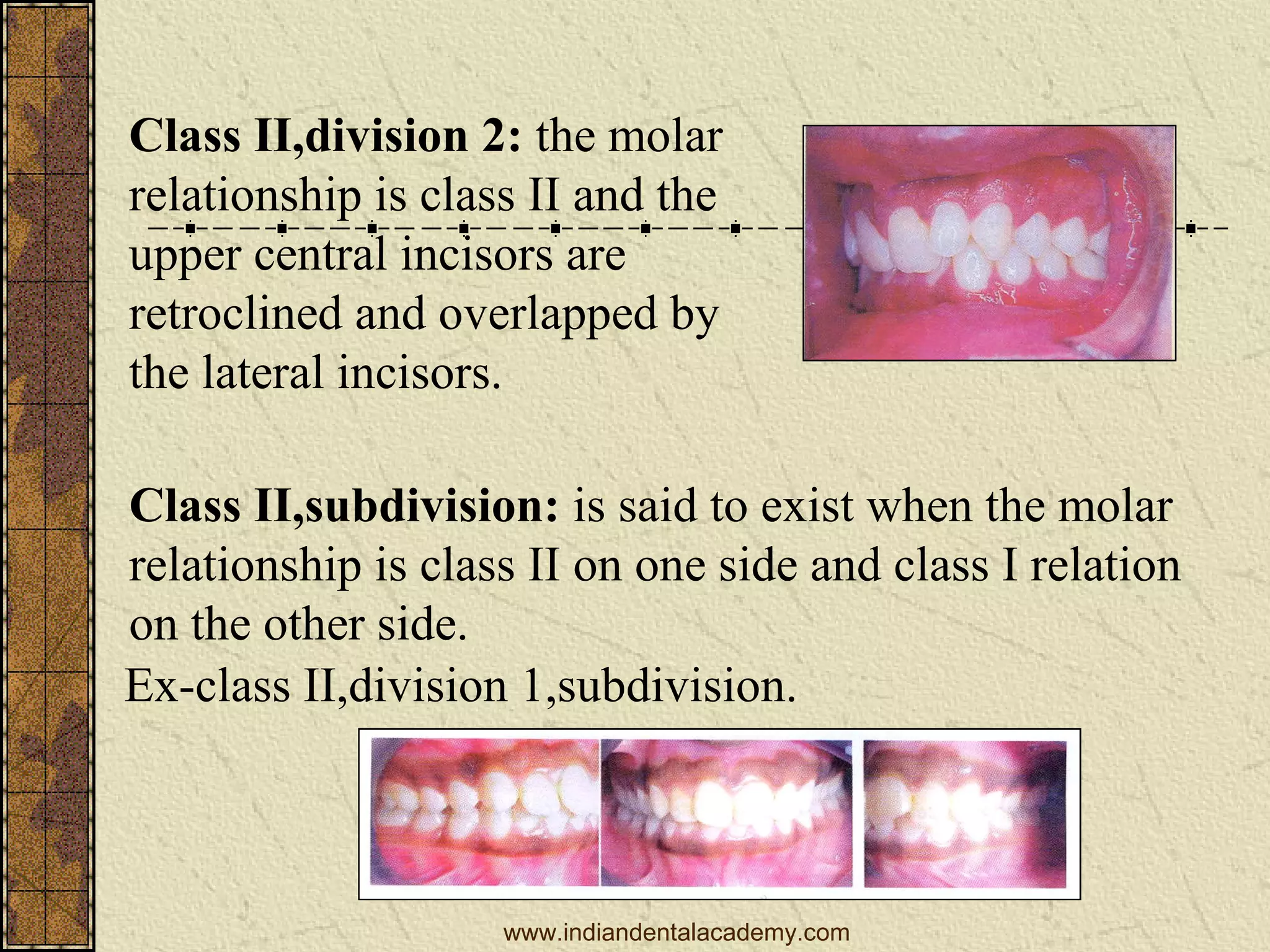
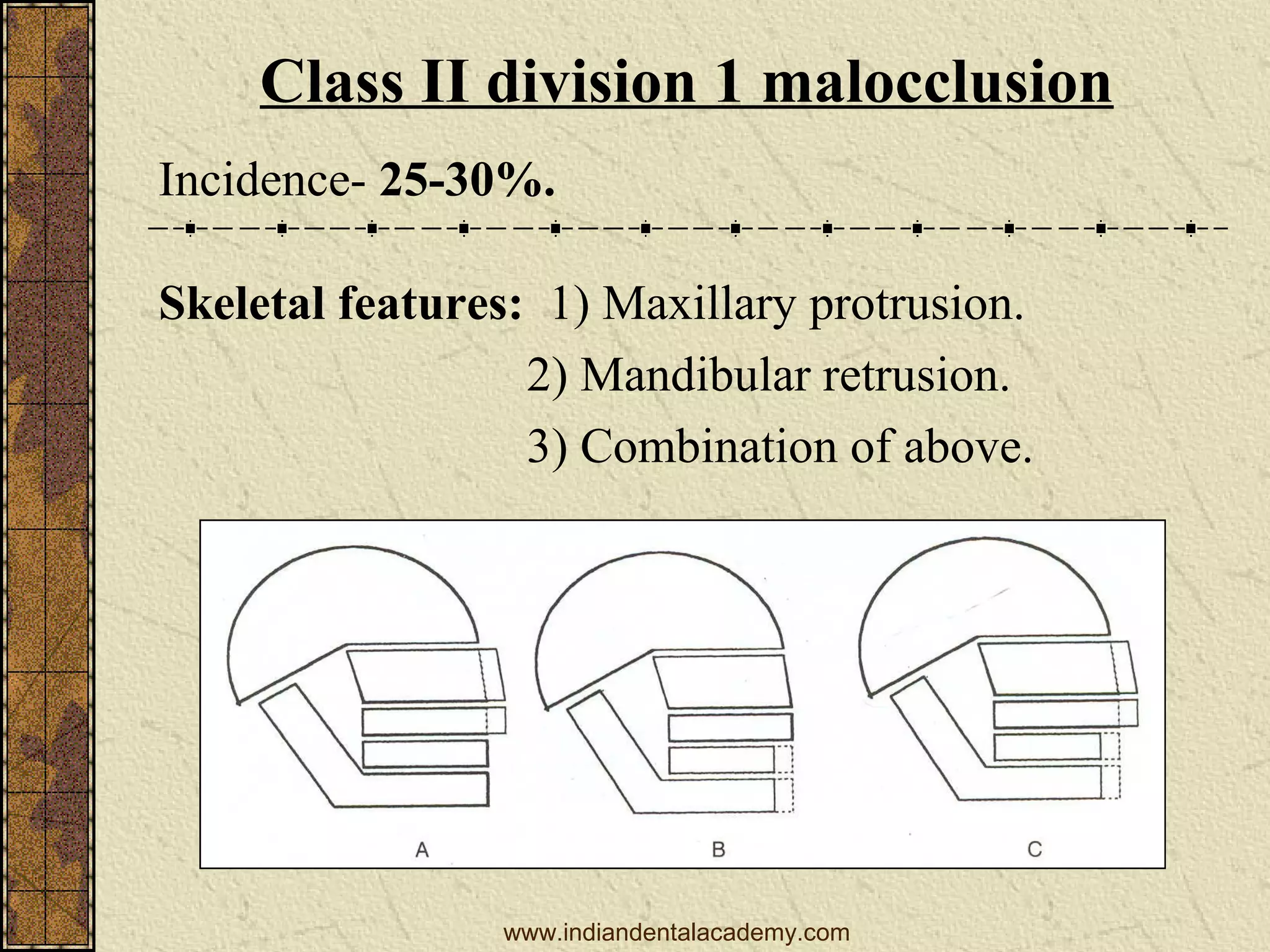
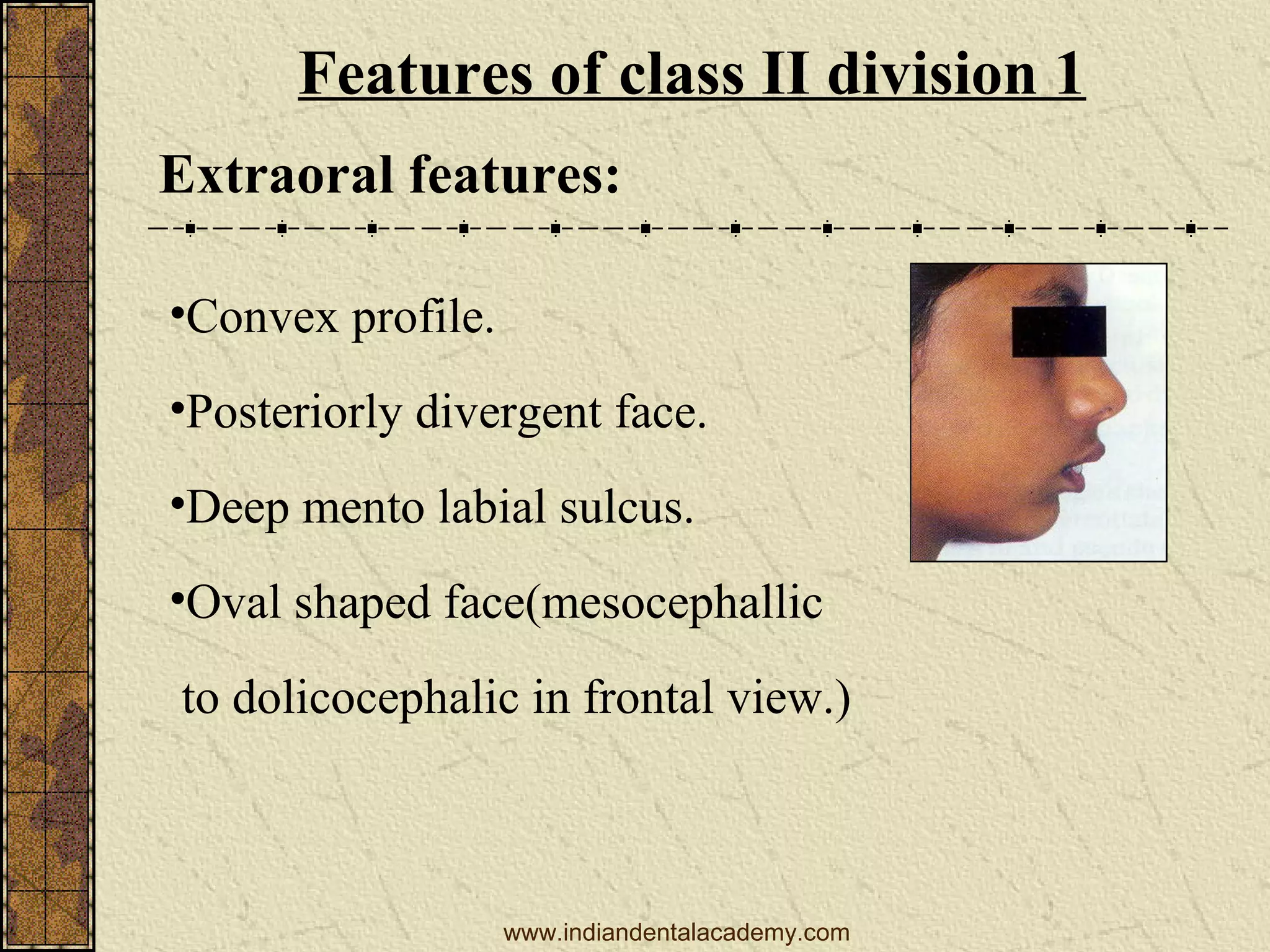
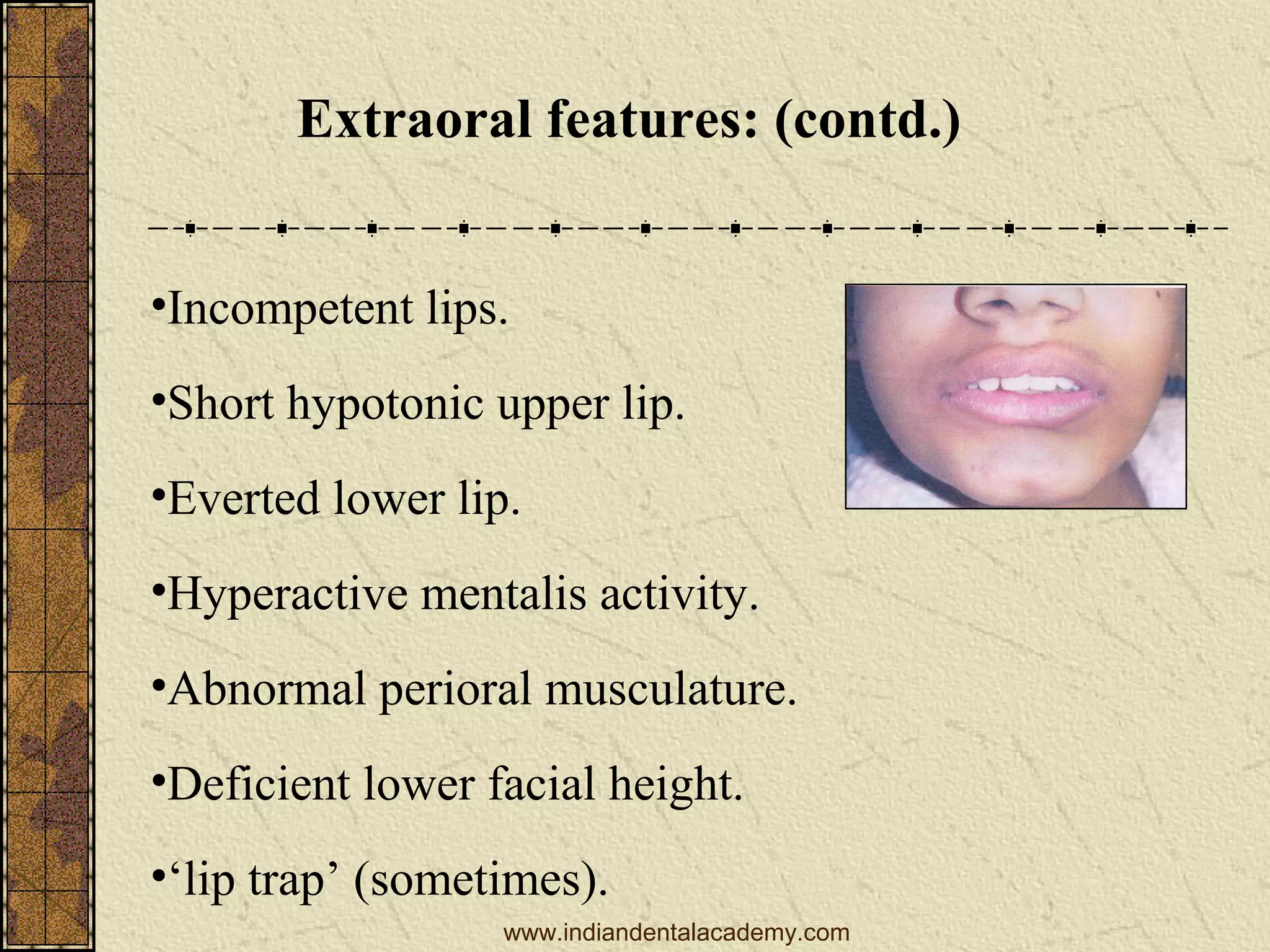
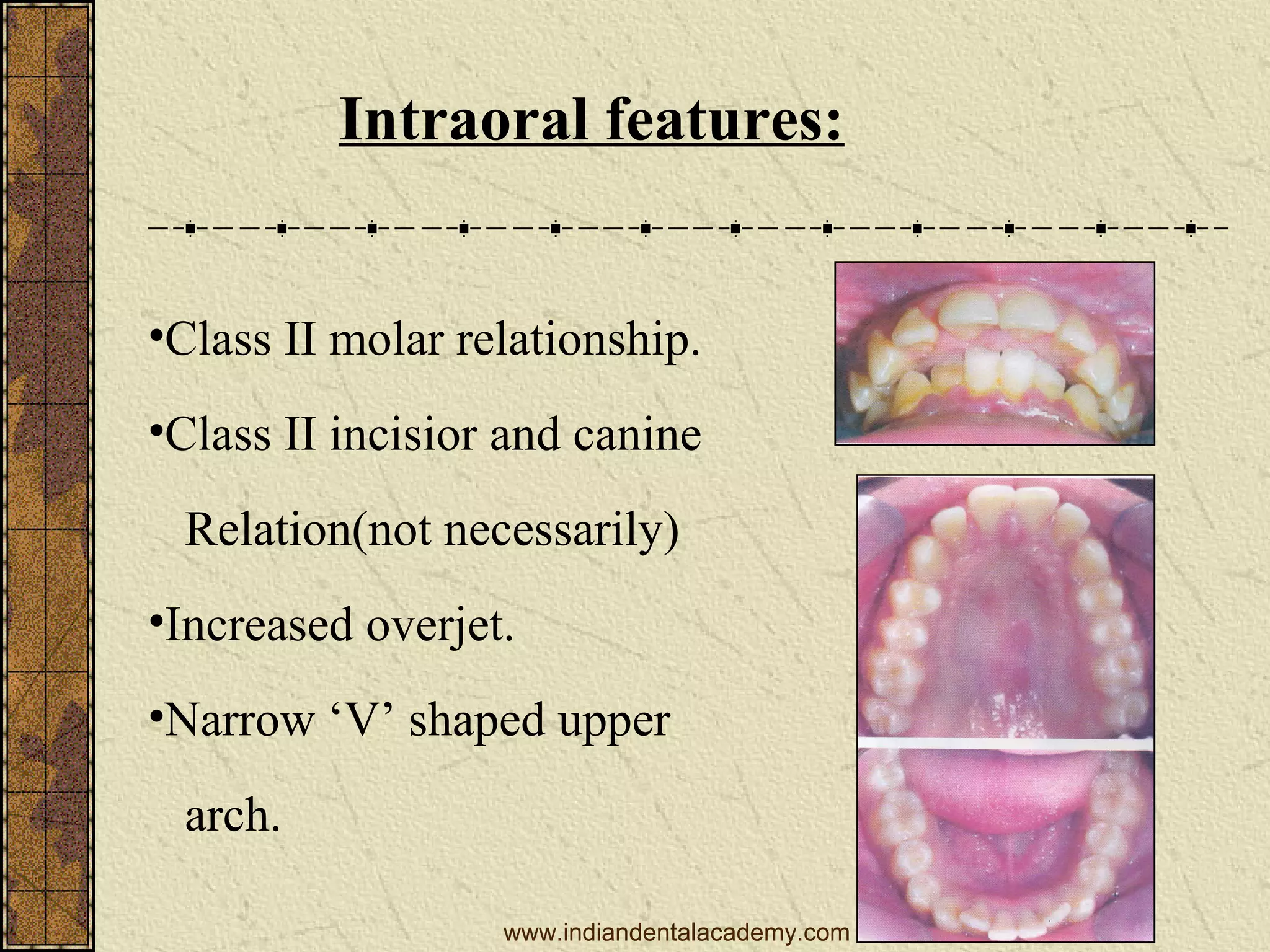
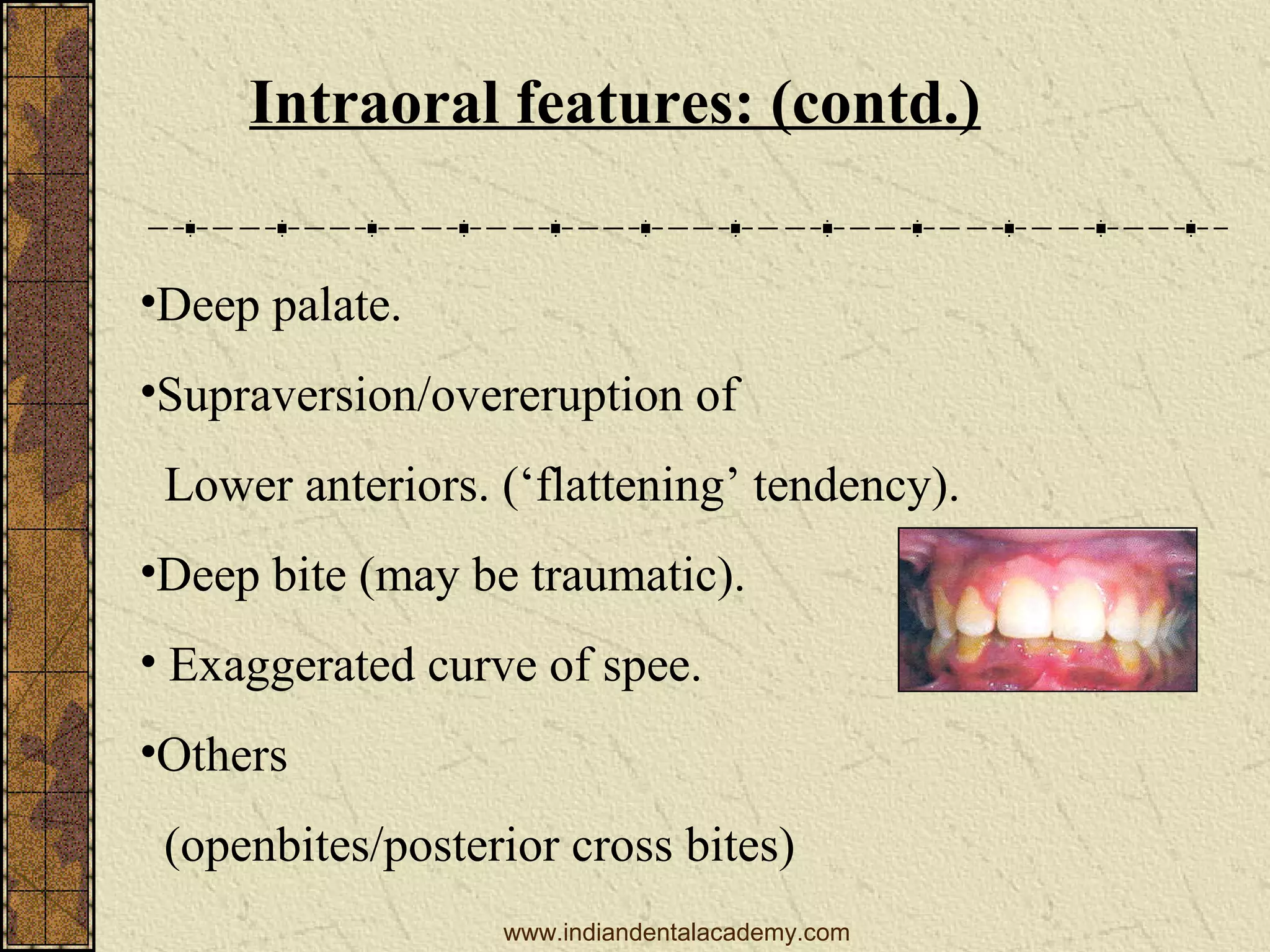
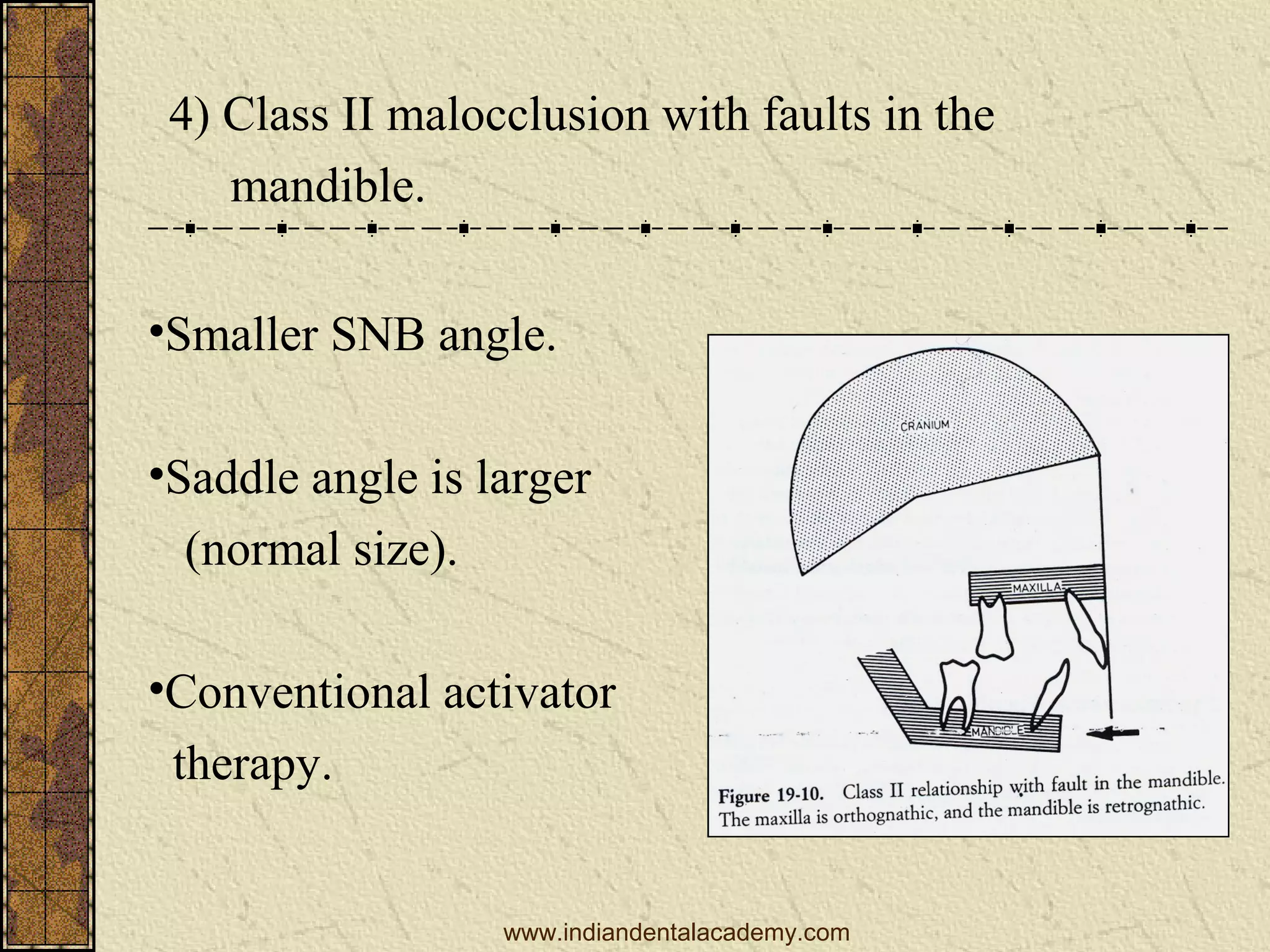


Class II malocclusion, categorized into two divisions by Angle's classification, involves a distal relationship of the mandibular arch to the maxilla. It presents various morphological classifications and features, including skeletal characteristics, etiological factors, extraoral and intraoral signs, and specific treatment approaches based on the patient's age and malocclusion type. Management can range from preventive measures and interceptive treatment during mixed dentition to surgical options for severe discrepancies in adults.