Downloaded 342 times
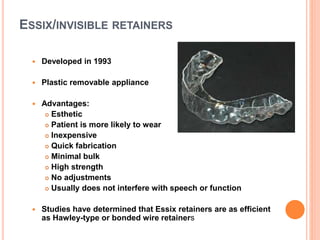
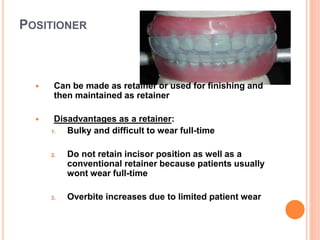
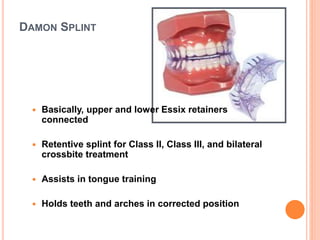


This document discusses various types of dental retention appliances. It begins by defining retention and explaining why it is necessary after orthodontic treatment. It then covers theories of retention, keys to eliminating lower retention, and classifications of retainers. The main types of retainers discussed are removable retainers like Hawley retainers, wrap-around retainers, and Essix retainers. Fixed retainers and principles of different retention times are also summarized.













































































