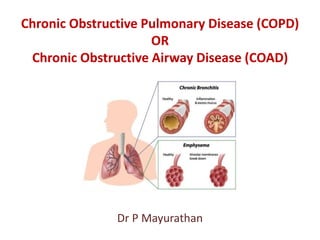
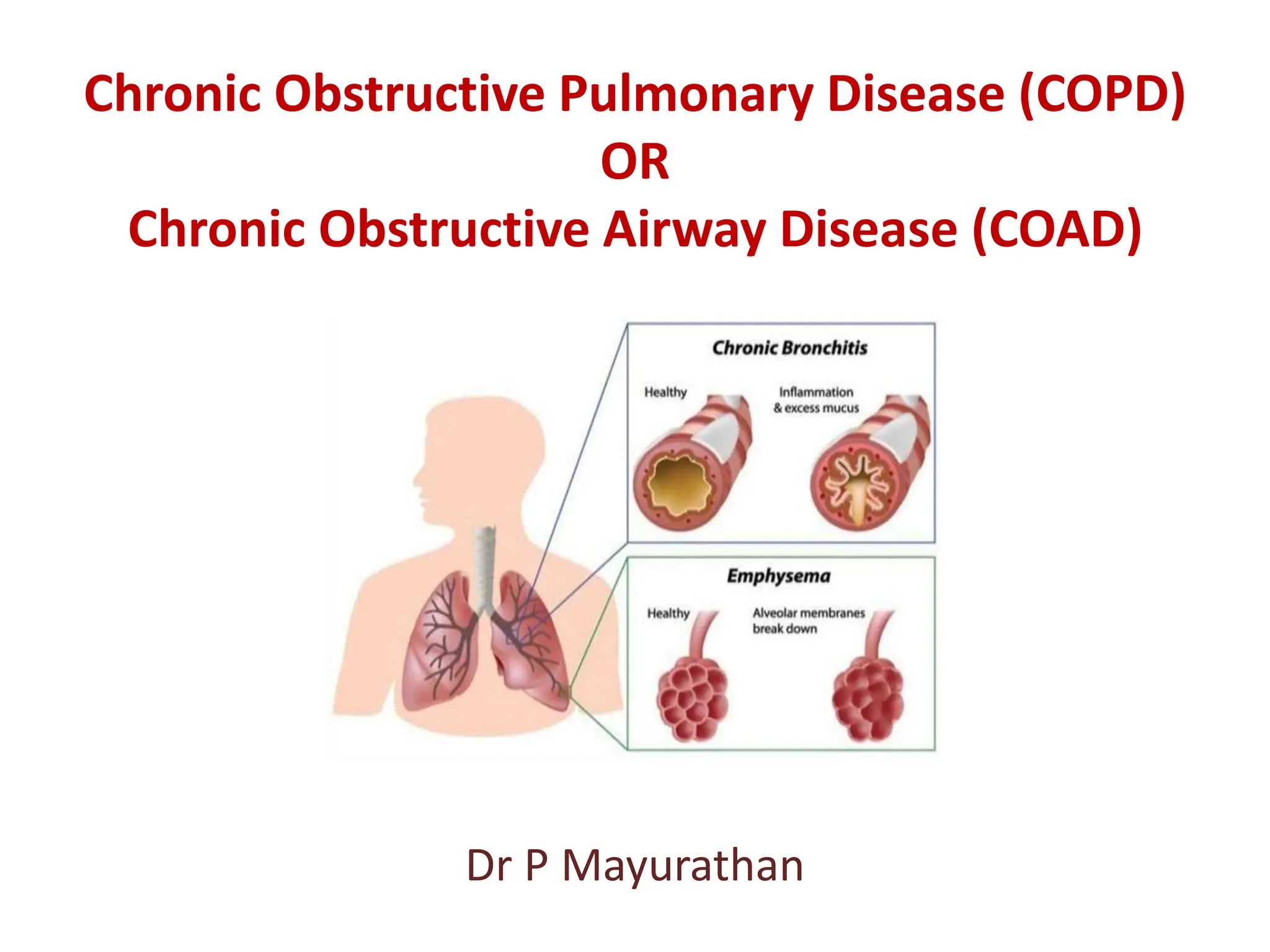
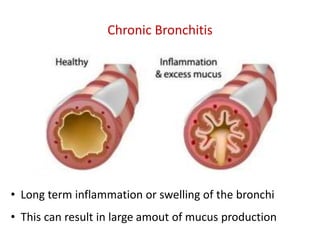
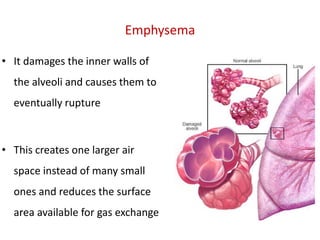
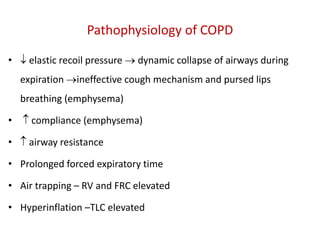
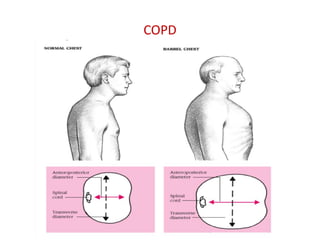
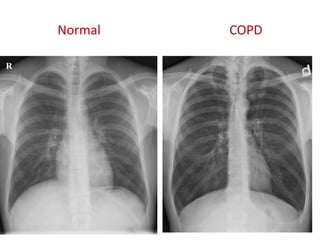
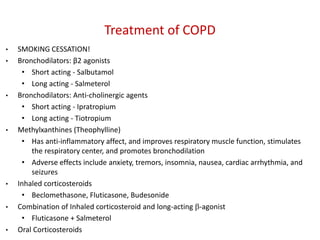
Chronic obstructive pulmonary disease (COPD) encompasses chronic bronchitis and emphysema, leading to airflow obstruction, chronic cough, and respiratory issues. Its prevalence is significant, with high smoking rates being a major risk factor, and it is the fourth leading cause of death in the USA. Treatment includes smoking cessation, bronchodilators, corticosteroids, oxygen therapy, and potential surgical options.


































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)


















