Download to read offline

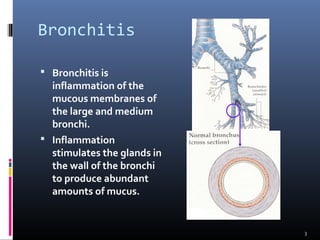
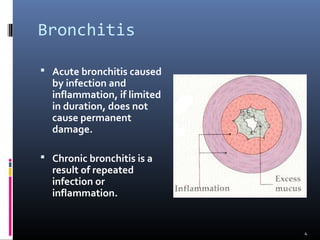





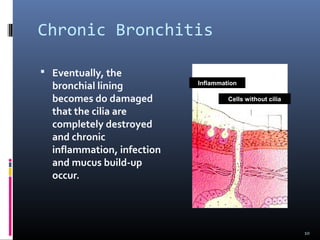





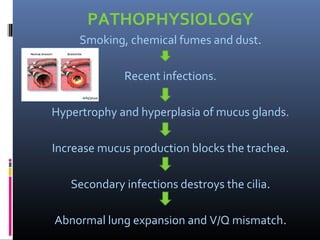










This document describes the structure and pathophysiology of chronic bronchitis. It begins by outlining the divisions of the airway passage from the trachea down to the alveolar sacs. It then explains that chronic bronchitis involves long-term inflammation and damage to the airways from repeated infection or irritants like cigarette smoke. This causes increased mucus production and loss of cilia function, leading to a buildup of retained mucus in the lungs. Over time, this causes further inflammation and lung damage. The document outlines symptoms, stages of exacerbation, and treatments for chronic bronchitis.