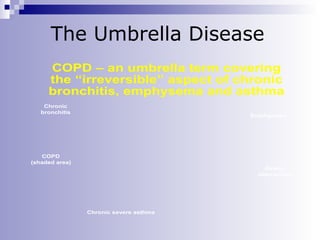
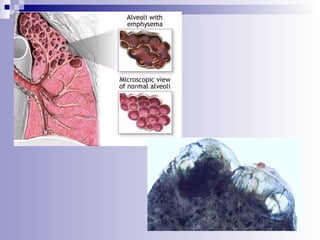
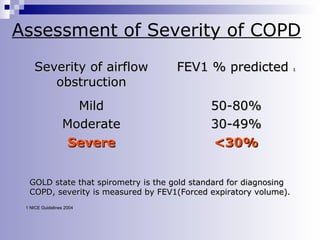
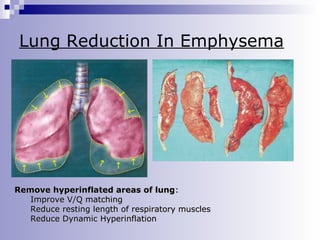
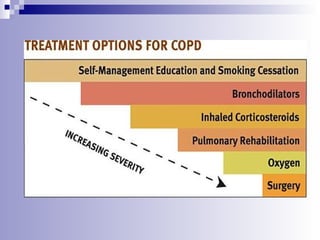
This document provides information on Chronic Obstructive Pulmonary Disease (COPD). It defines COPD as a disease characterized by persistent airflow limitation that is usually progressive. The primary cause of COPD is tobacco smoking. It discusses the characteristics and components of COPD including chronic bronchitis and emphysema. The document also covers the diagnosis, assessment of severity, management including medications, oxygen therapy, pulmonary rehabilitation, and end of life care considerations for COPD patients.