Downloaded 195 times






























![LGL LeukemiaLGL Leukemia
Two types:
–T cell type [80%]
[CD 2,3,5,7,8,16, 56+ & 4, 57-]
–NK cell type](https://image.slidesharecdn.com/chronicleukemias-csbrp-151030075550-lva1-app6892/75/Chronic-leukemias-csbrp-40-2048.jpg)





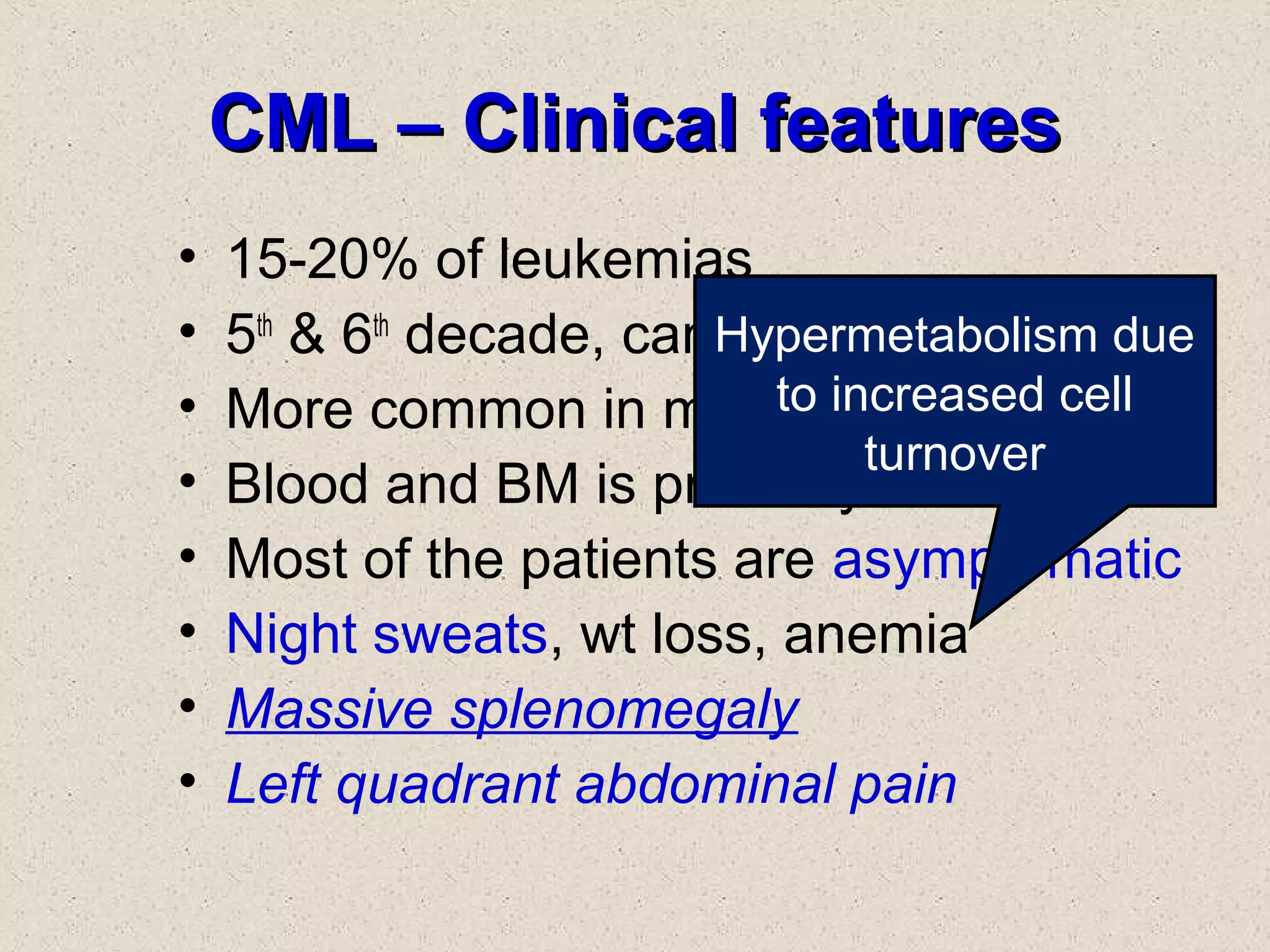
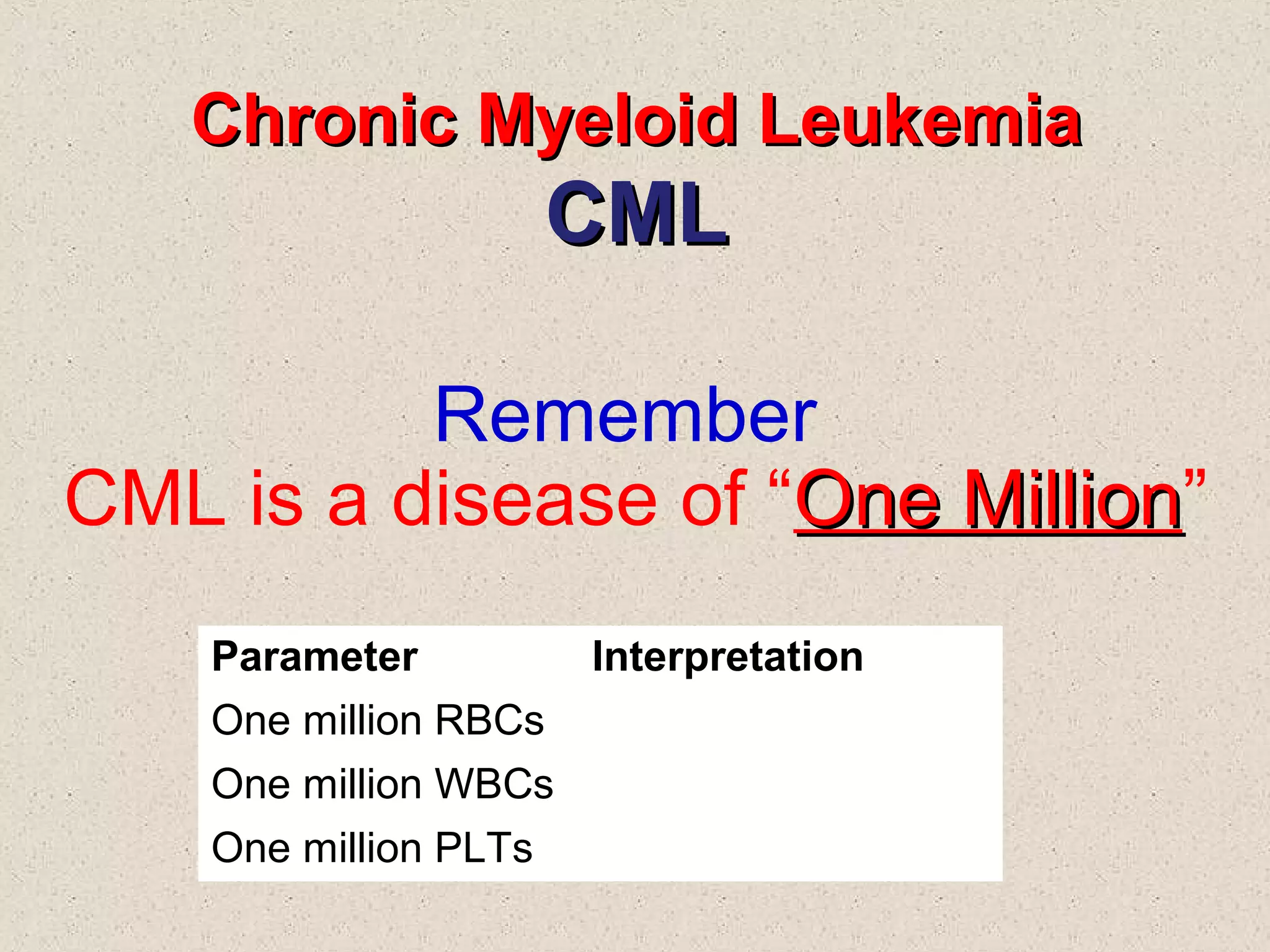




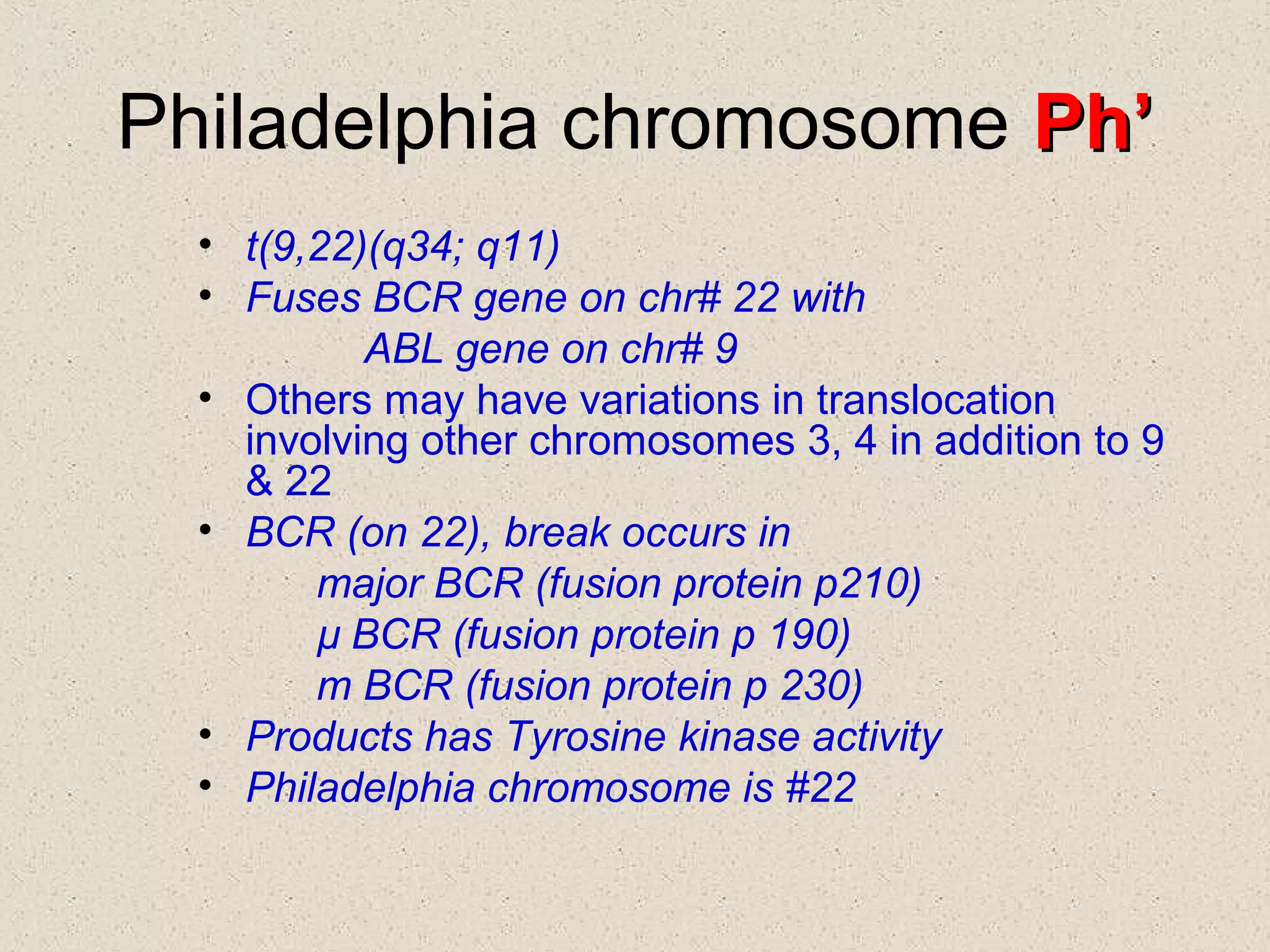


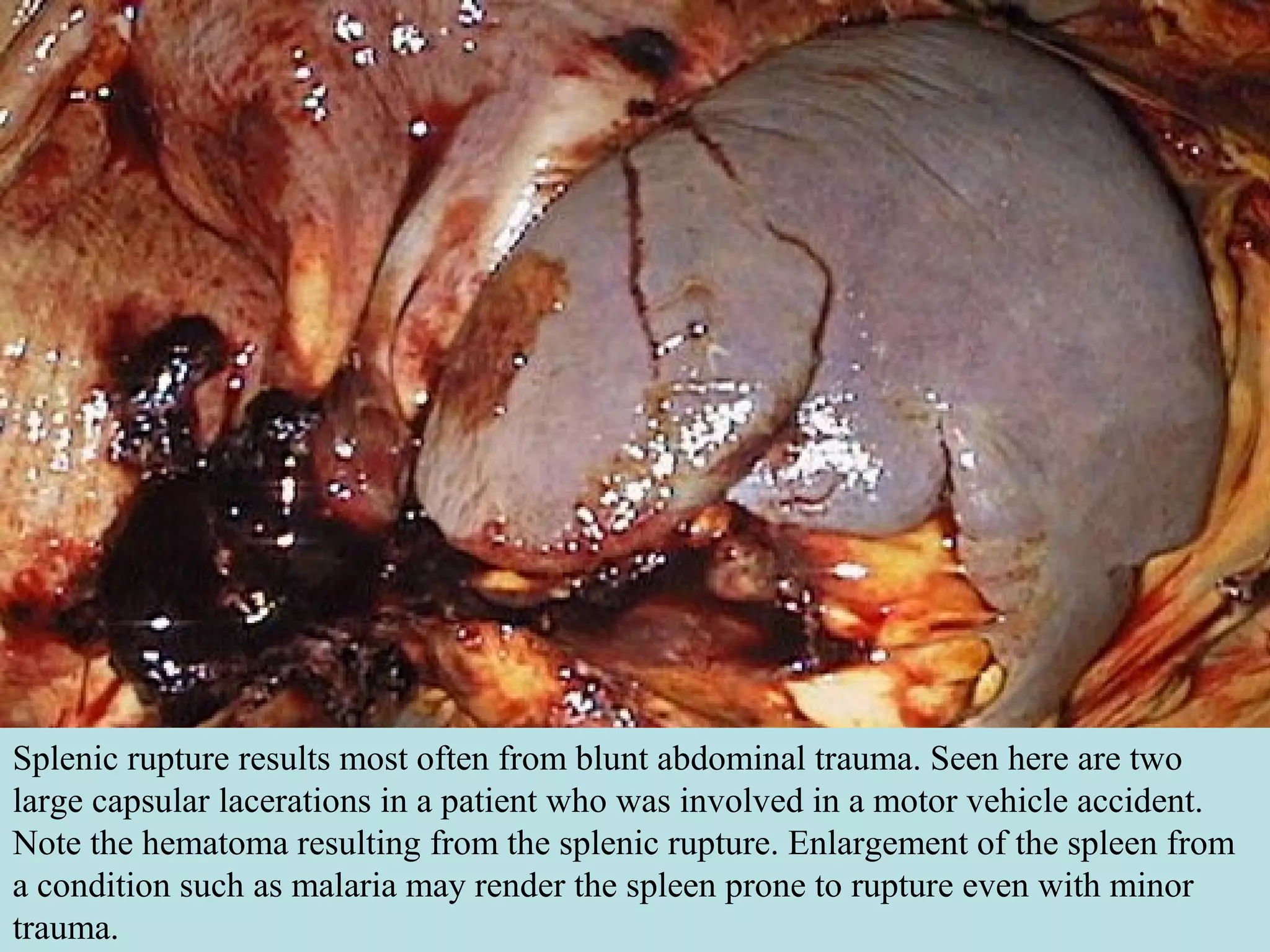

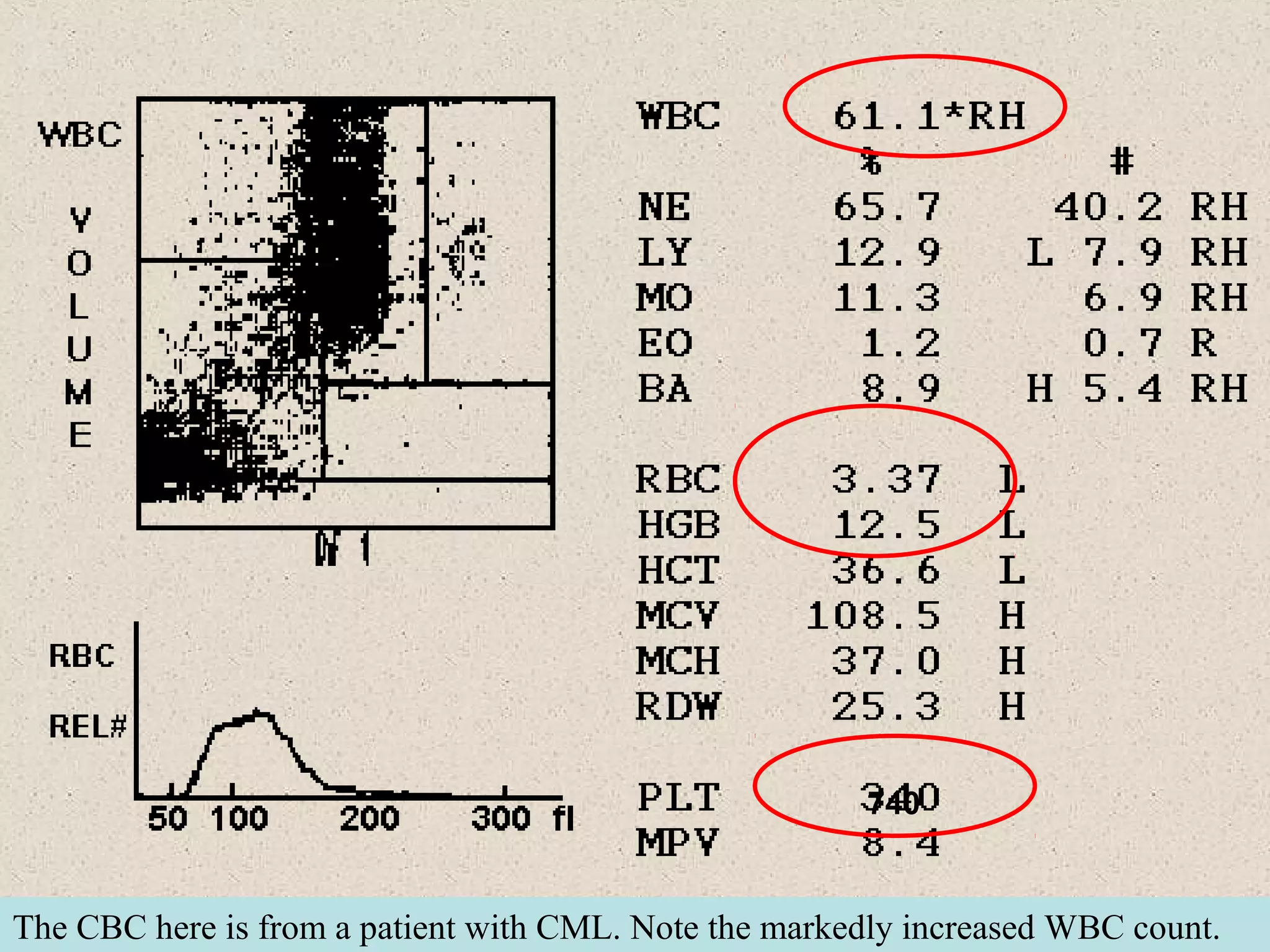
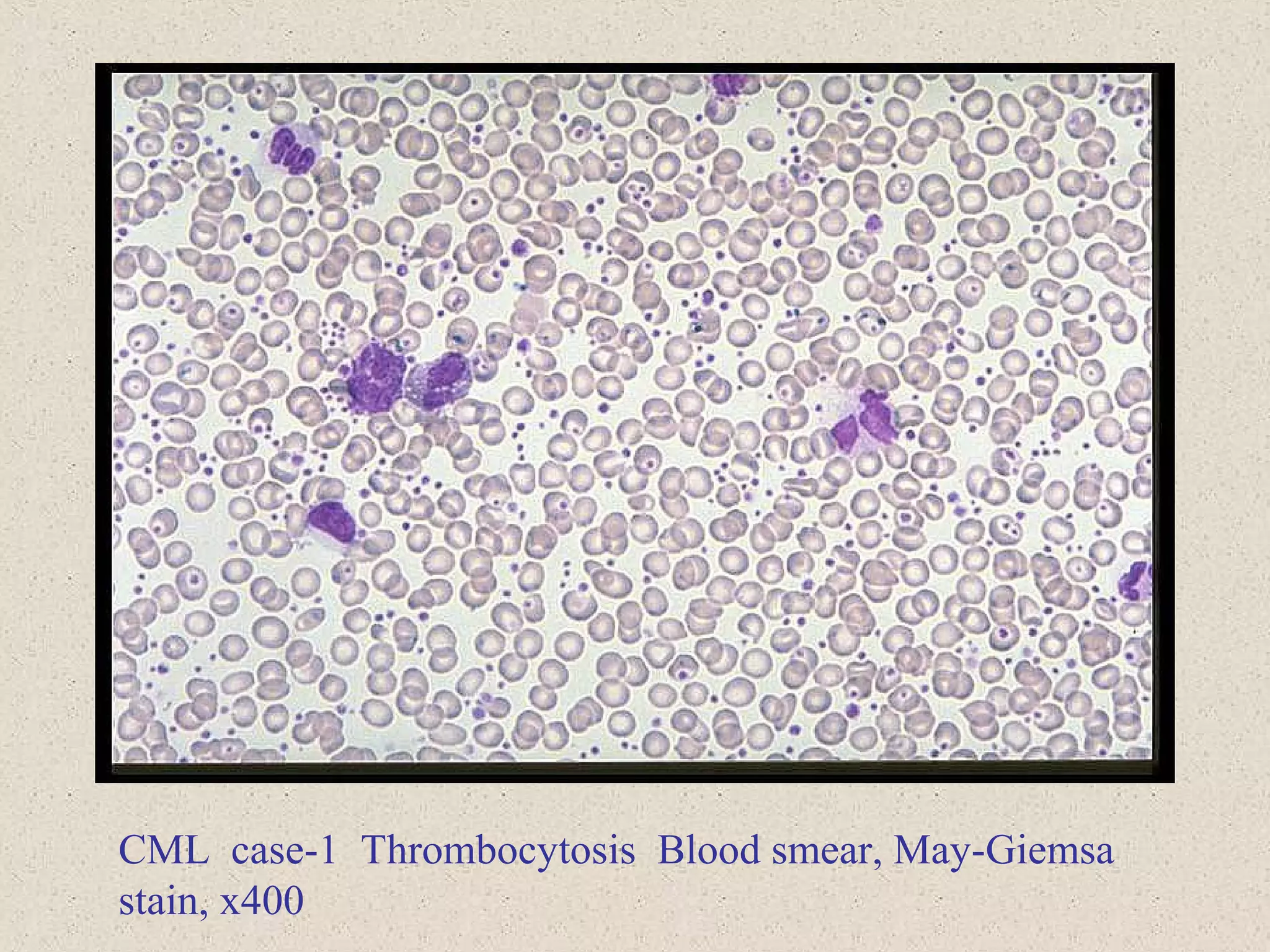

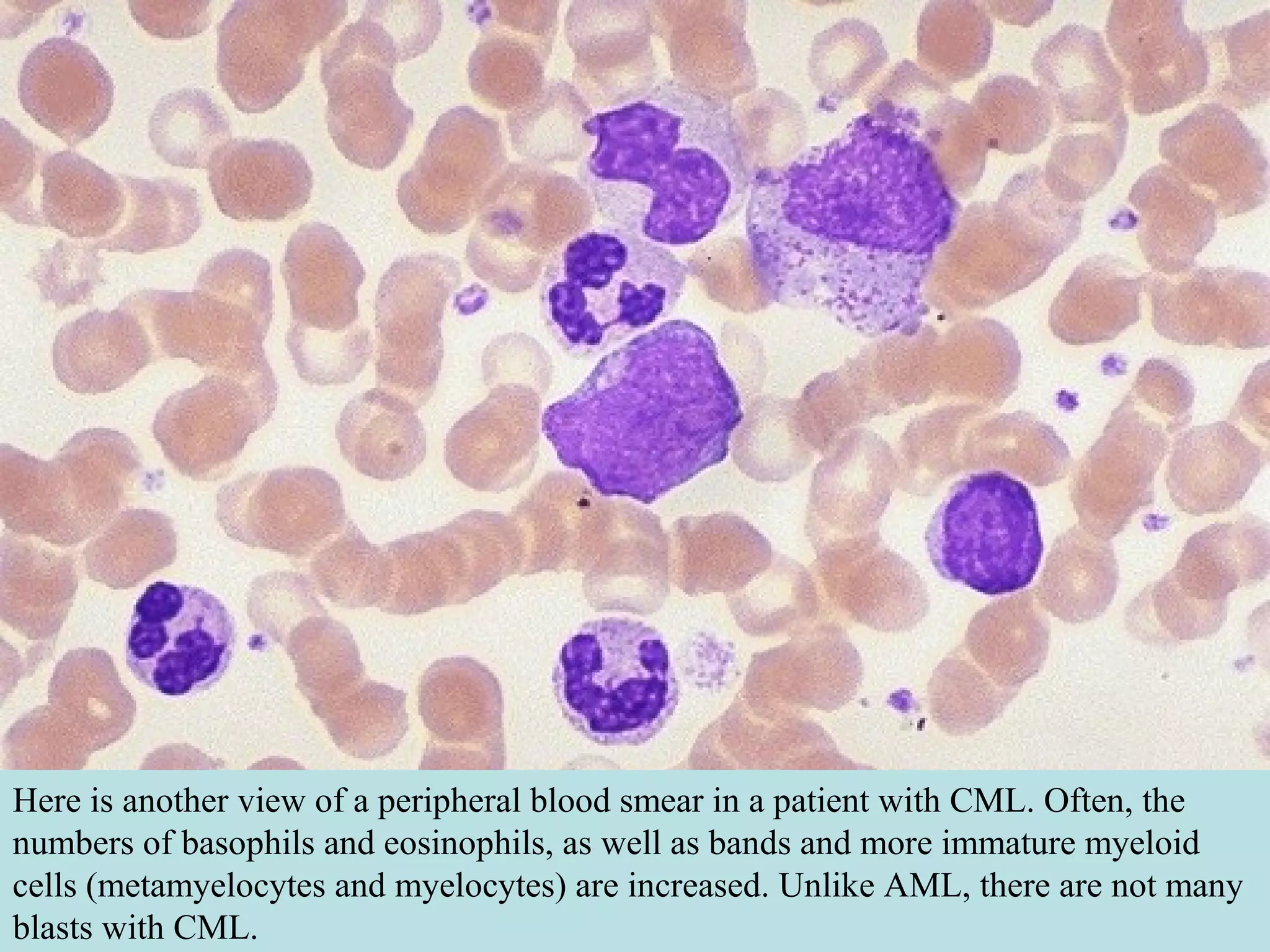


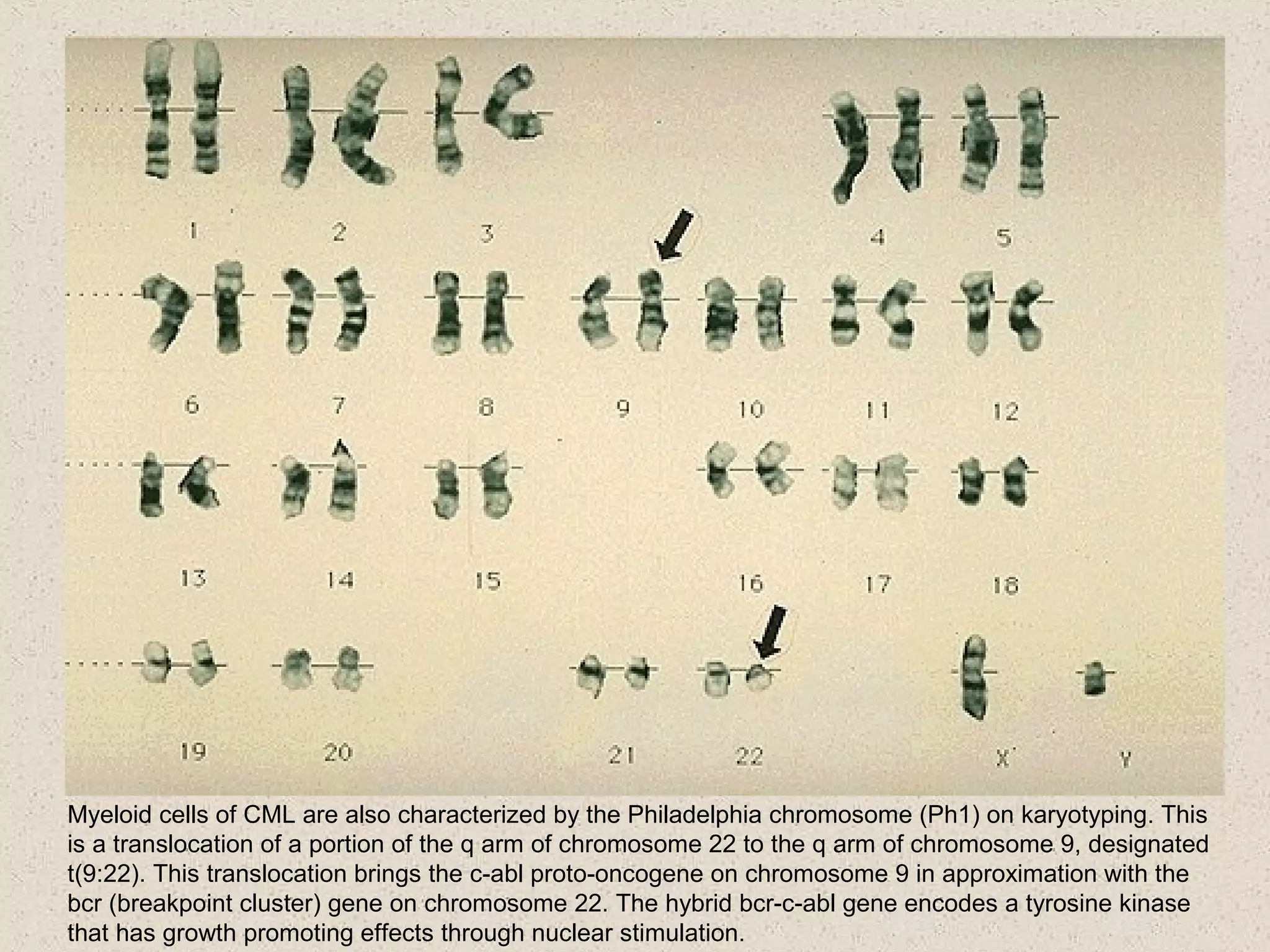








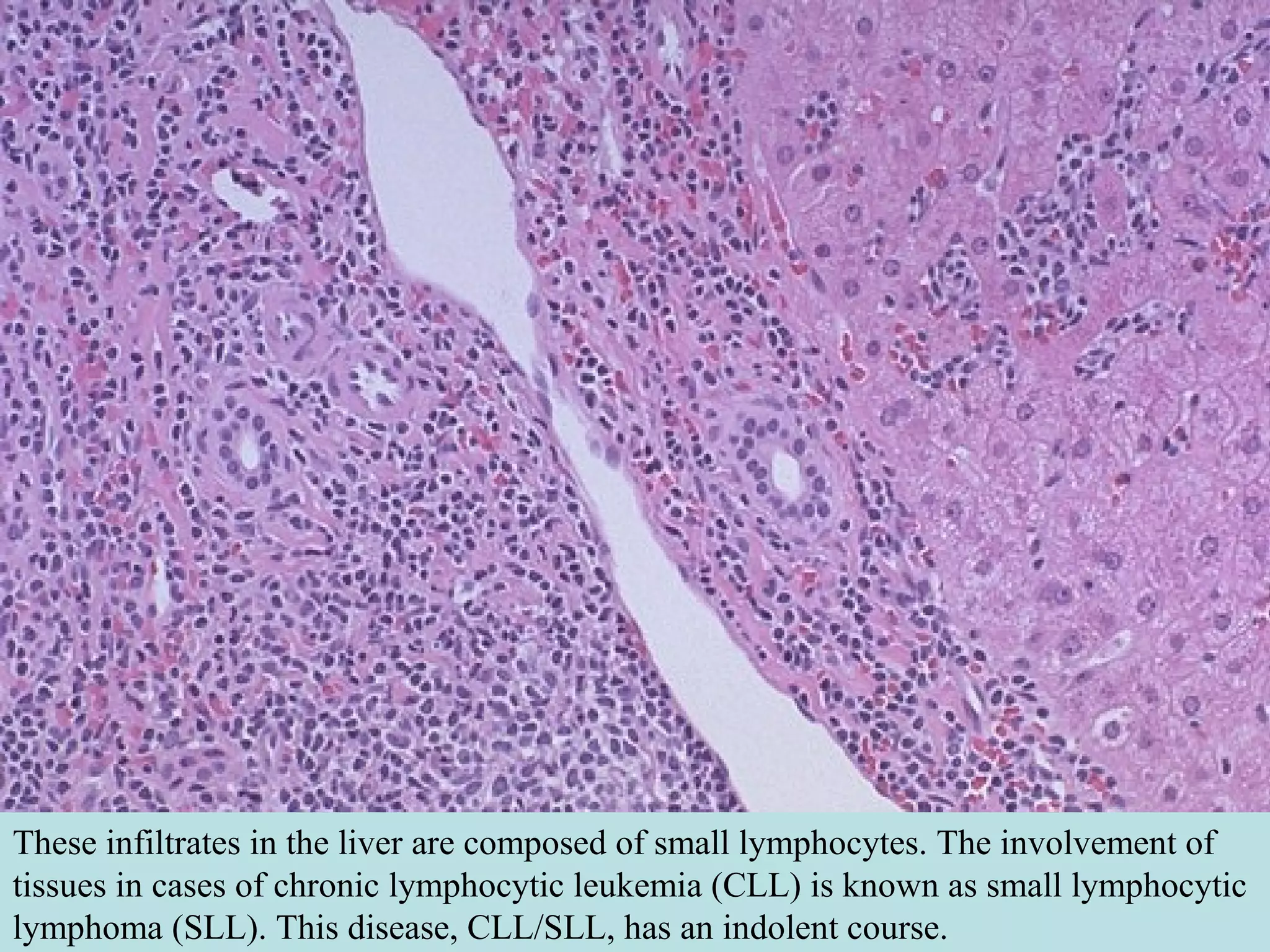
This document discusses chronic leukemias and myeloproliferative disorders including chronic myeloid leukemia (CML) and myelofibrosis. CML is distinguished from other myeloproliferative disorders by the presence of the Philadelphia chromosome and BCR-ABL fusion gene. CML is characterized by leukocytosis, thrombocytosis, and anemia. It progresses through chronic, accelerated, and blast phases defined by increasing blast counts and symptoms. The massive spleen seen in CML is indicative of the underlying myeloproliferative process.






























































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)












