Downloaded 1,080 times

![WHAT IS CKD ?
National Kidney Foundation (NKF) defines CKD as
evidence of renal damage (based on abnormal UA
[proteinuria, hematuria] or
structural abnormalities (found with US) or
GFR < 60 mL/min for 3 or more months](https://image.slidesharecdn.com/chronickidneydiseasebydrbeenish-140713054148-phpapp01/75/Chronic-Kidney-Disease-CKD-2-2048.jpg)
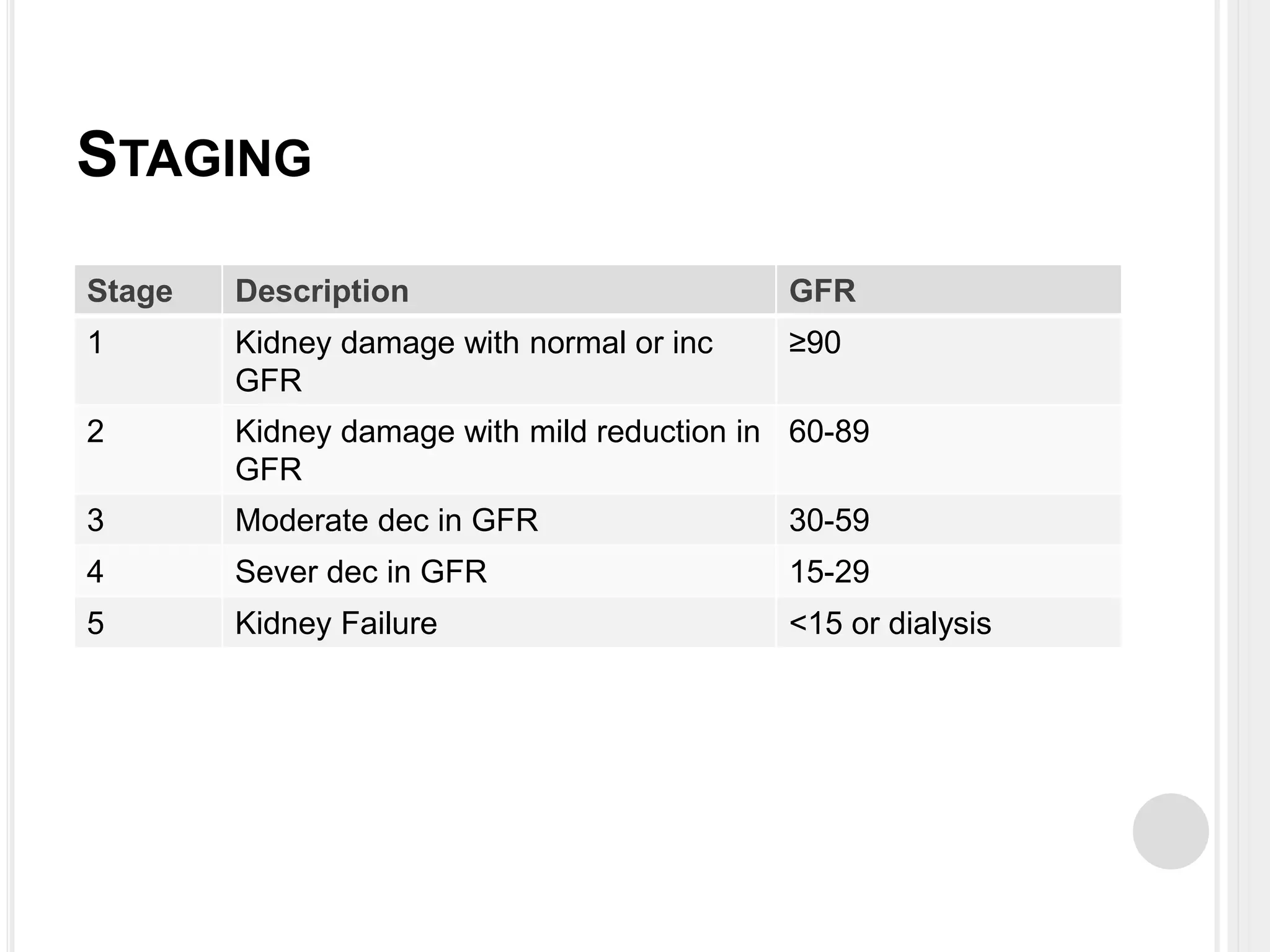






















Chronic kidney disease (CKD) is a progressive decline in renal function, characterized by reduced clearance of solutes and significant retention in body fluids. The disease is staged based on glomerular filtration rate (GFR), with various causes including diabetic kidney disease, hypertension, and glomerular disease. Management involves controlling blood pressure, addressing complications such as anemia and bone metabolism disorders, and considering dialysis in advanced cases.























































































