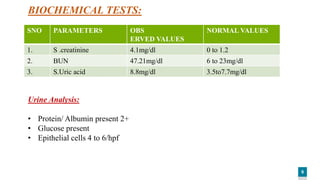
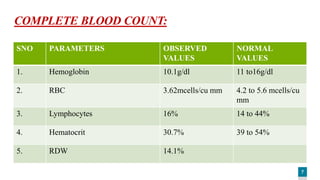
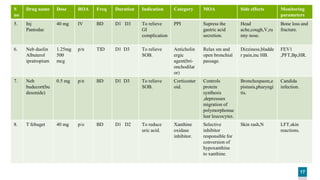
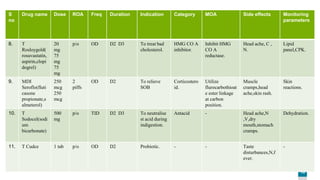
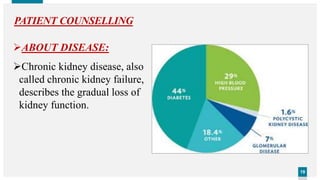
The document presents a case study of a 60-year-old male patient diagnosed with chronic kidney disease (CKD), driven by diabetes and hypertension. It includes a SOAP analysis that details the patient's symptoms, objective findings, biochemical tests, and management plan, which encompasses medications and lifestyle modifications. The assessment indicates that the patient's renal function is severely compromised, necessitating interventions like dialysis or a kidney transplant.

















































![12. a case study on ckd stage 5 [kidney failure]](https://cdn.slidesharecdn.com/ss_thumbnails/12-200326130709-thumbnail.jpg?width=640&height=640&fit=bounds)





















