Downloaded 26 times

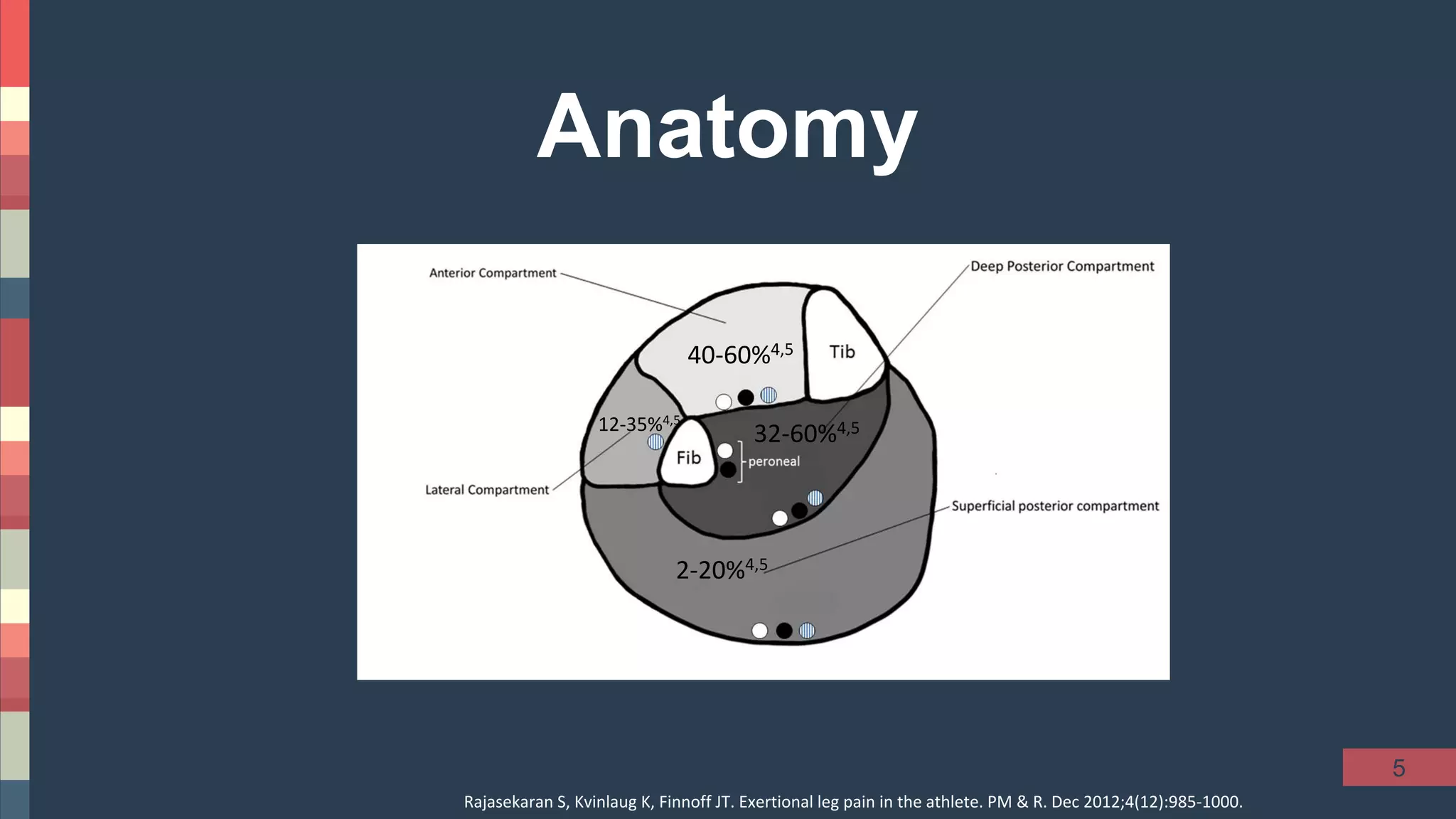
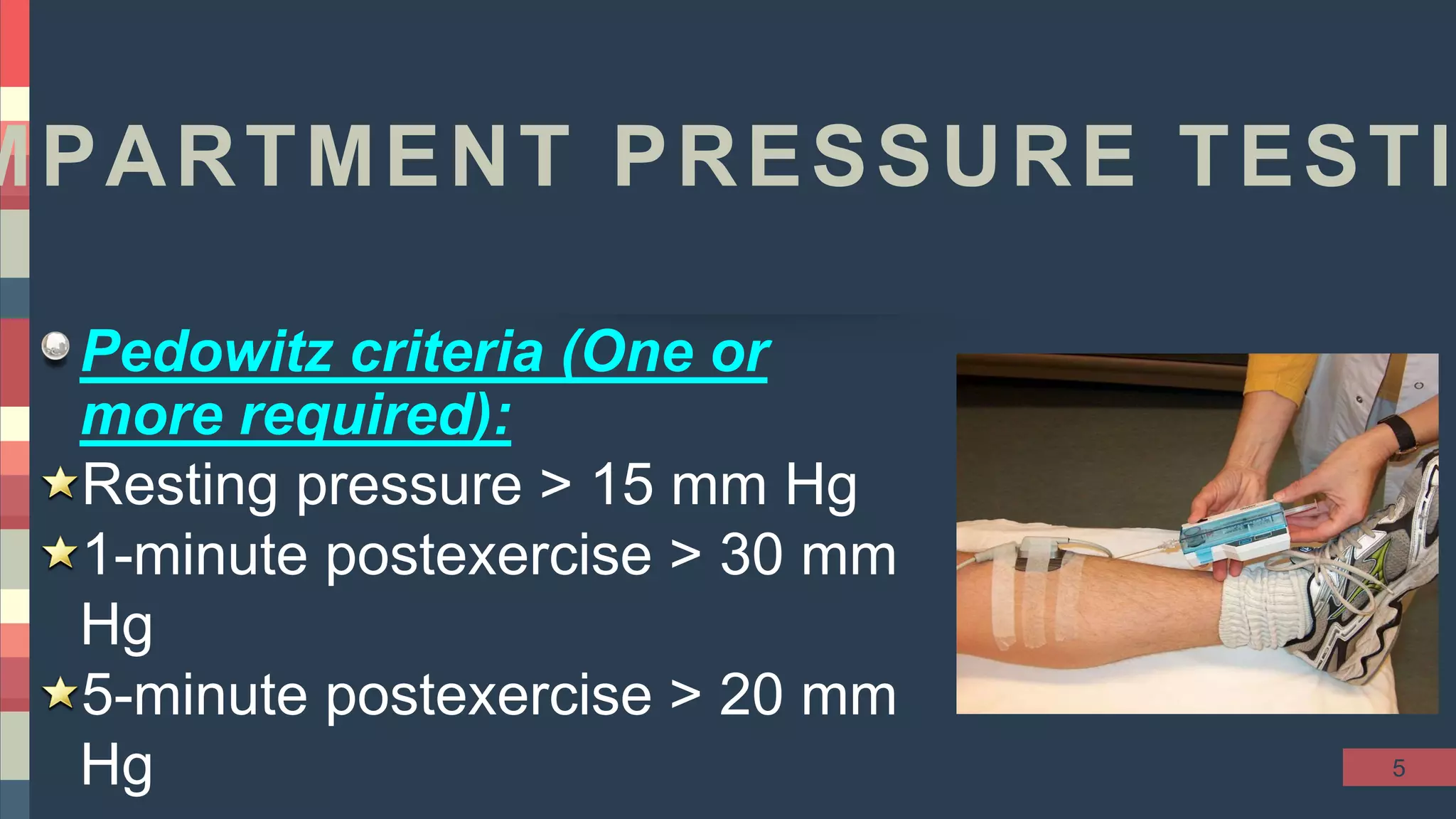




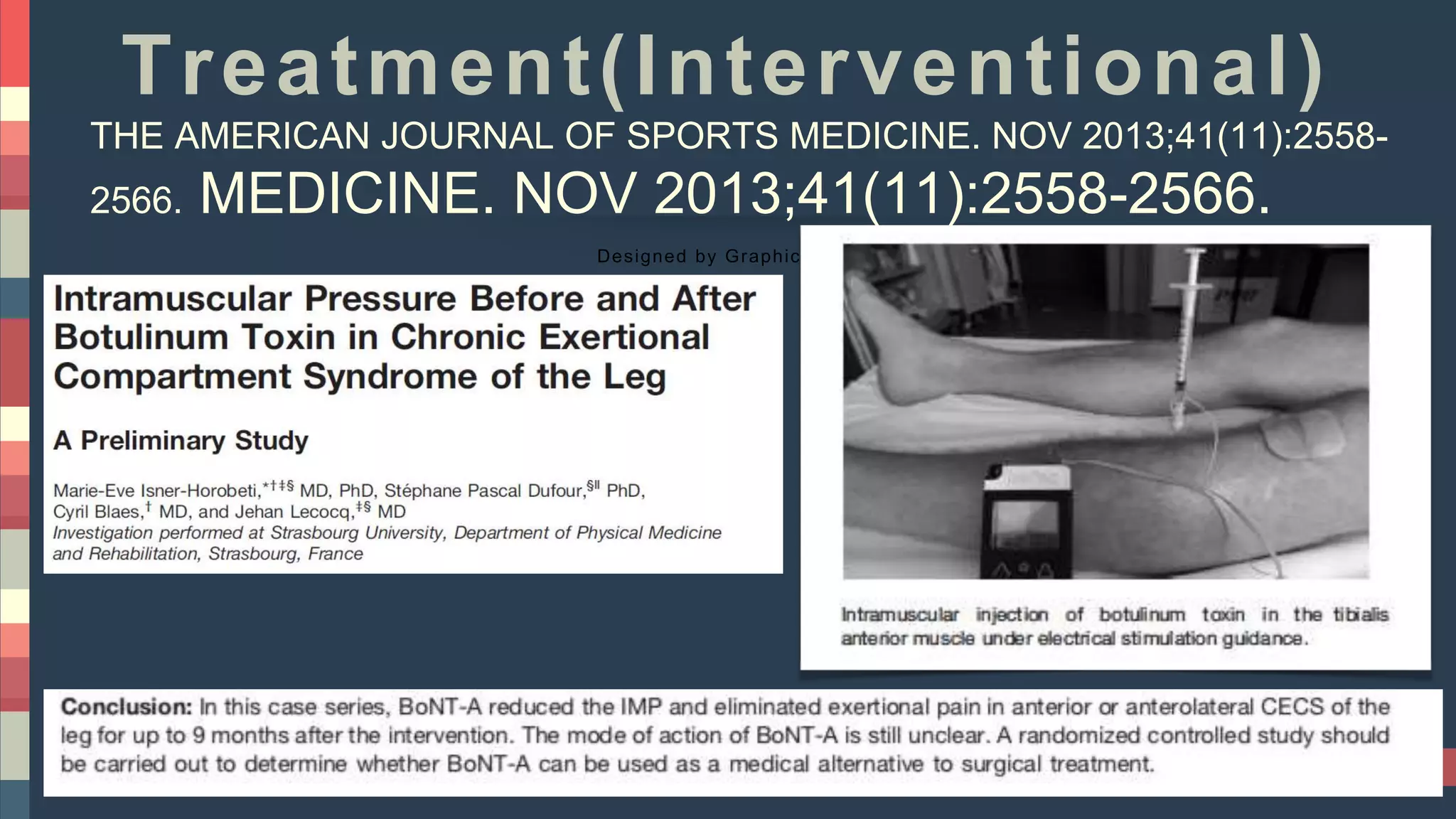







Chronic exertional compartment syndrome (CECS) is characterized by reversible ischemia in a noncompliant muscle compartment that causes pain with exercise but resolves with rest. It most commonly affects the anterior compartment of the lower leg in young, competitive runners and military recruits. The pain is exercise-induced and worsens over 20-30 minutes of running before resolving within 15-30 minutes of stopping. Diagnosis involves clinical evaluation for tenderness over the affected muscles and compartment pressure testing at rest and after exercise. Treatment begins with activity modification, but refractory cases may require fasciotomy to release the tight fascia.













































































