Downloaded 22 times

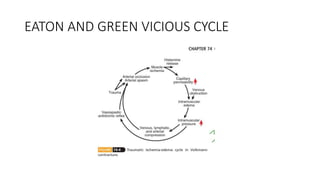
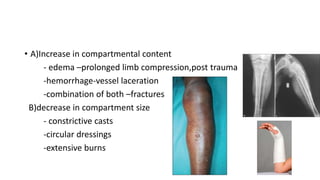
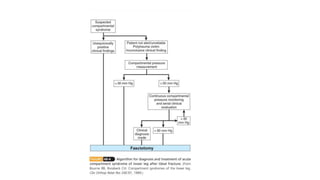


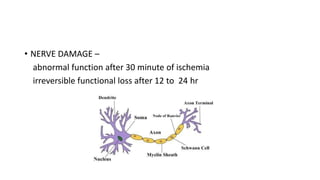
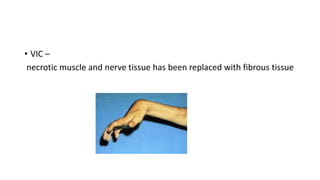


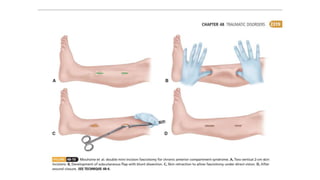

The document provides a comprehensive overview of compartment syndrome, defining it as elevated interstitial pressure in a closed compartment that compromises microvascular function. It discusses the types (acute and chronic), pathophysiology, etiology, clinical evaluation, diagnosis, and management strategies, including both nonoperative and operative treatments. Complications and outcomes of the condition, as well as specific information on chronic exertional compartment syndrome, are also addressed.
















































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)


















