Downloaded 51 times
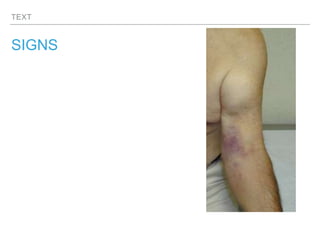
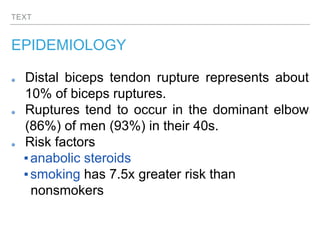

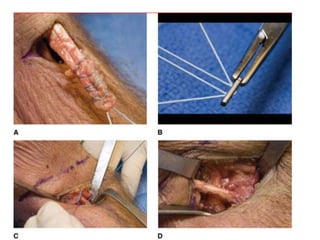
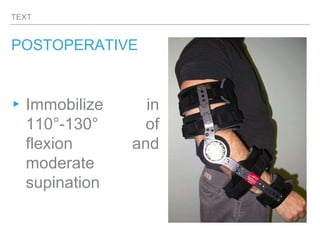


This document discusses the case of a 39-year-old male weightlifter who experienced a painful pop in his elbow followed by inability to carry things, consistent with a distal biceps tendon rupture. Distal biceps tendon ruptures typically occur in dominant arms of men in their 40s during eccentric loading. Surgical repair is usually recommended for young, active patients to restore function, with fixation techniques like suture buttons providing the strongest repair. Postoperative rehabilitation involves immobilization in flexion and supination.







































![Tip & tricks [Autosaved] - Copy.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/tiptricksautosaved-copy-220902124657-5a096dbd-thumbnail.jpg?width=640&height=640&fit=bounds)





































