Discharge from leftear
• Insidious onset
• Gradually Progressive
• purulent in nature
• yellowish in color
• Continuous
• Scanty to moderate in amount
• Foul smelling
• Occasionally Blood Mixed
• Partially relieved on topical medications
• No aggravating factor
5.
Decreased hearing fromleft ear
• Insidious in onset
• Gradually progressive
• Non fluctuant
• have difficulty in using mobile phone from left ear
• Difficulty hearing and localizing sound when called from left side or
behind
6.
No history of
•Ear ache
• High grade fever
• Headache, Nausea, vomiting
• Loss of consciousness
• Neck stiffness/photophobia
• Abnormal body movements
• Tinnitus ,vertigo
Past history
No H/osimilar illness in the past
No h/o DM/Bronchial asthma,PTB
No History of Head and Neck surgeries or Malignancy
9.
Family History
No h/osimilar illness in family member
No h/o PTB/DM/HTN/Bronchial asthma
No History of Head and Neck surgeries or Malignancy
10.
Personal History
Student
lives infamily of 4 members
Consumes mixed diet
Bowel/bladder/sleep/appetite -Normal
No Habit of putting oil in ear/ bathing in ponds
11.
Drug History
History oftaking topical ear drops on and off.
Allergic History
No h/o allergy to drugs or known substances.
12.
GENERAL PHYSICAL EXAMINATION
Generalexamination
Patient is conscious, cooperative,average built and well oriented to
time, place and person
Pulse: 68 bpm, regular, normal rate, rhythm, volume and character, no RR
delay, all peripheral pulses palpable.
Blood Pressure: 110/70 mm Hg in right arm in sitting position
Respiratory Rate: 20 breaths per minute
Temp: 97.4°F, axillary
Systemic Examination
CNS :Grossly intact
Respiratory:
B/L Normal vesicular breath sounds
No added sounds
CVS: S1, S2 heard,
No murmur
Abdomen:
Soft, non tender
No organomegaly
Bowel sound heard
15.
Ear
• Pinna: Bilateralpinna normal in shape, size, angle, position
• Tragal tenderness: absent
• Circumduction tenderness: absent
• 3 finger test: absent
16.
Pre auricular Region
NoScar/sinus/ swelling/ discharges or
tenderness
Post auricular Region
No Scar/sinus/ swelling/ discharges or
tenderness
Retroauricular groove:
Not Obliterated
17.
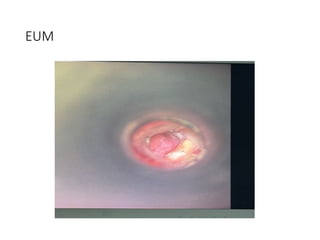
External Auditory Meatus
B/LPatent
No Discharge
External Auditory Canal: without speculum and
with Speculum
Right Left
Roof
Anterior wall
Posterior wall
Floor
wnl
purulent
discharge on EAC
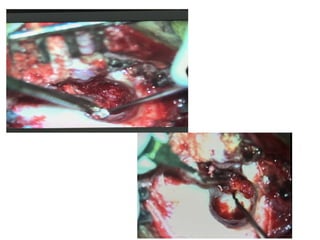
• Patient underwent
LeftModified Radical Mastoidectomy with Type III tympanoplasty
With Temporalis Fascia Grafting via postaural approach under General
Anesthesia
#32 The Towne view is an angled anteroposterior radiograph of the skull and visualizes the petrous part of the pyramids, the dorsum sellae and the posterior clinoid processes, which are visible in the shadow of the foramen magnum
Schuller's view is a lateral radiographic view of skull principally used for viewing mastoid cells