Downloaded 26 times
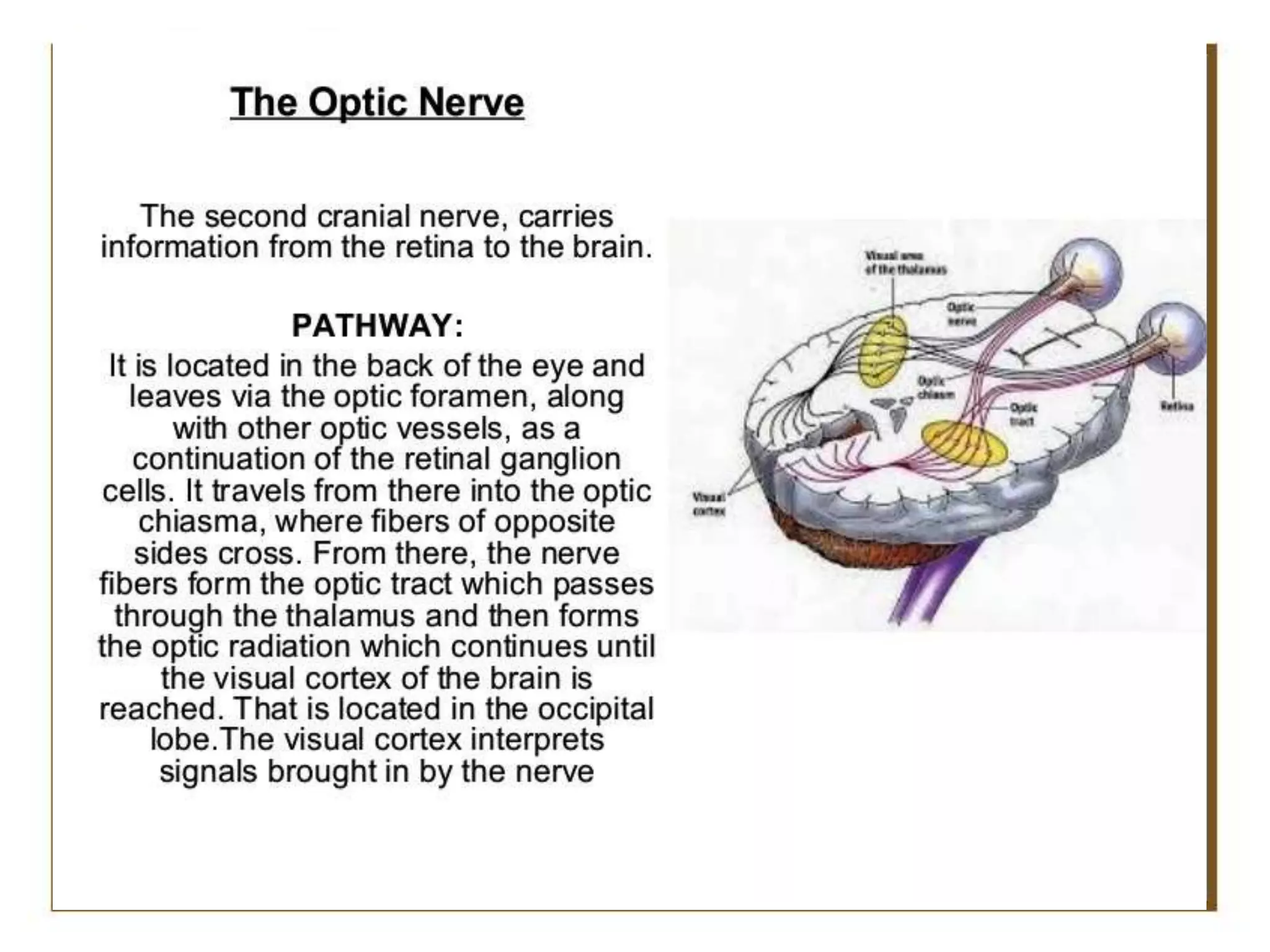
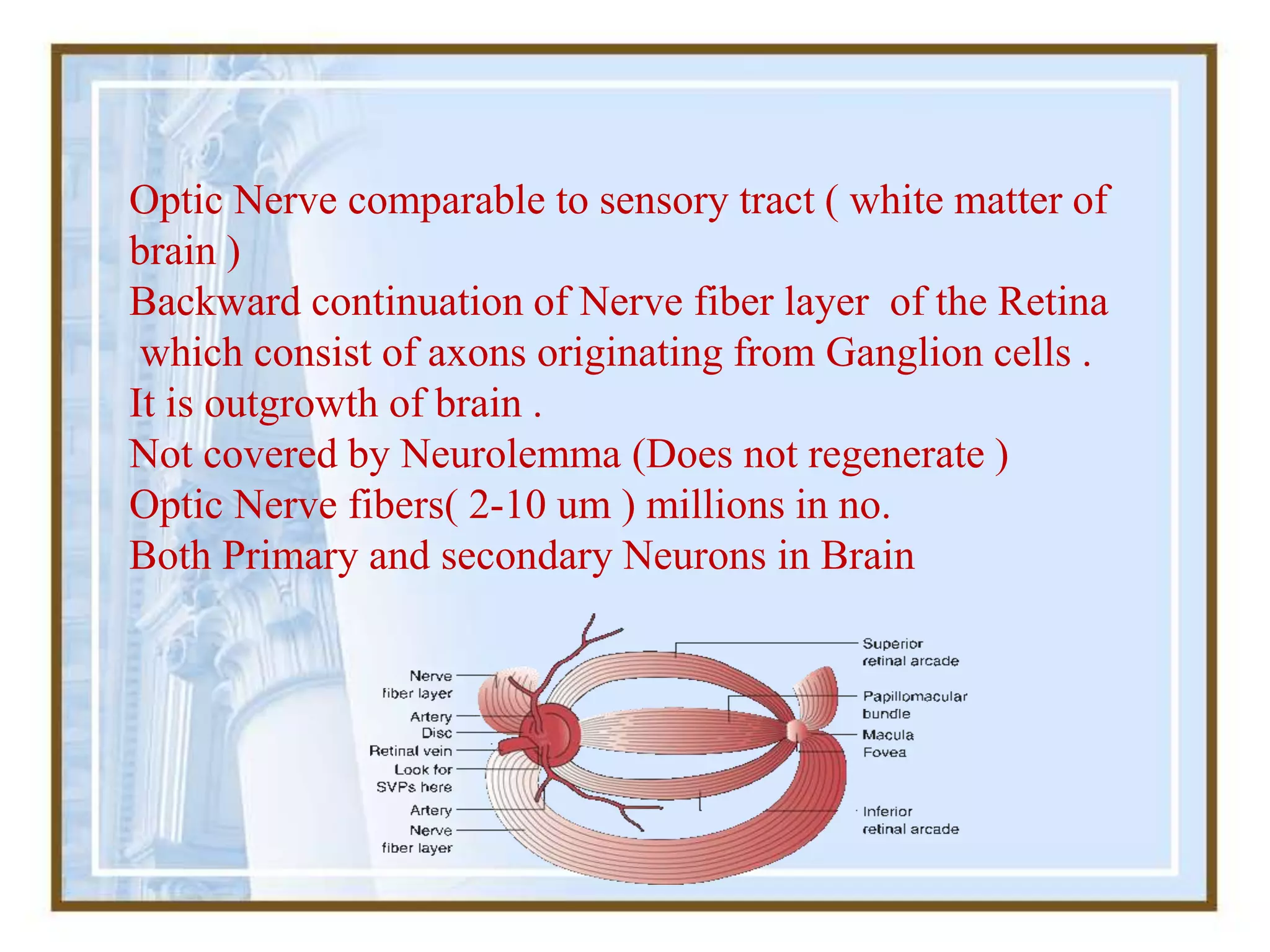
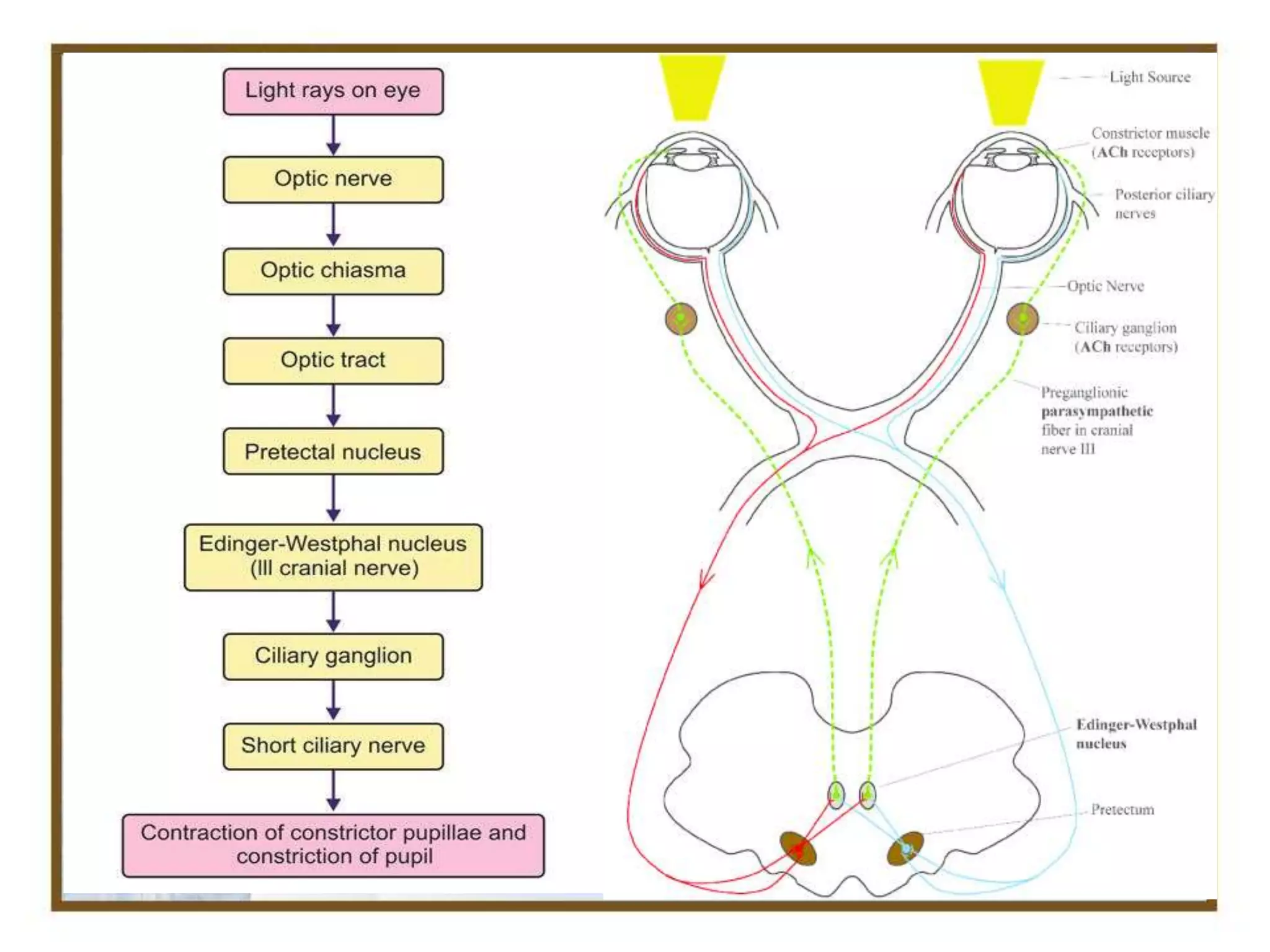
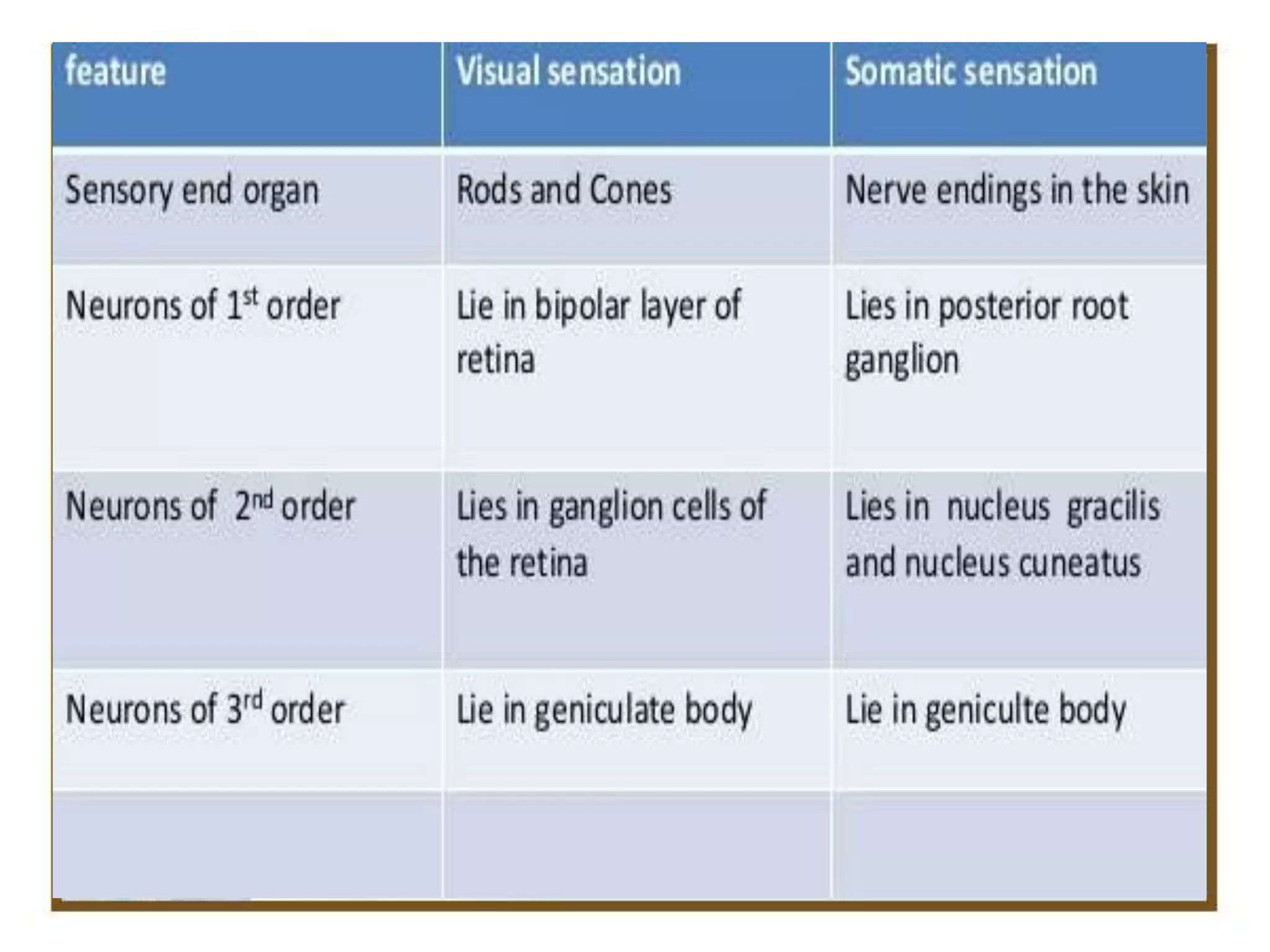
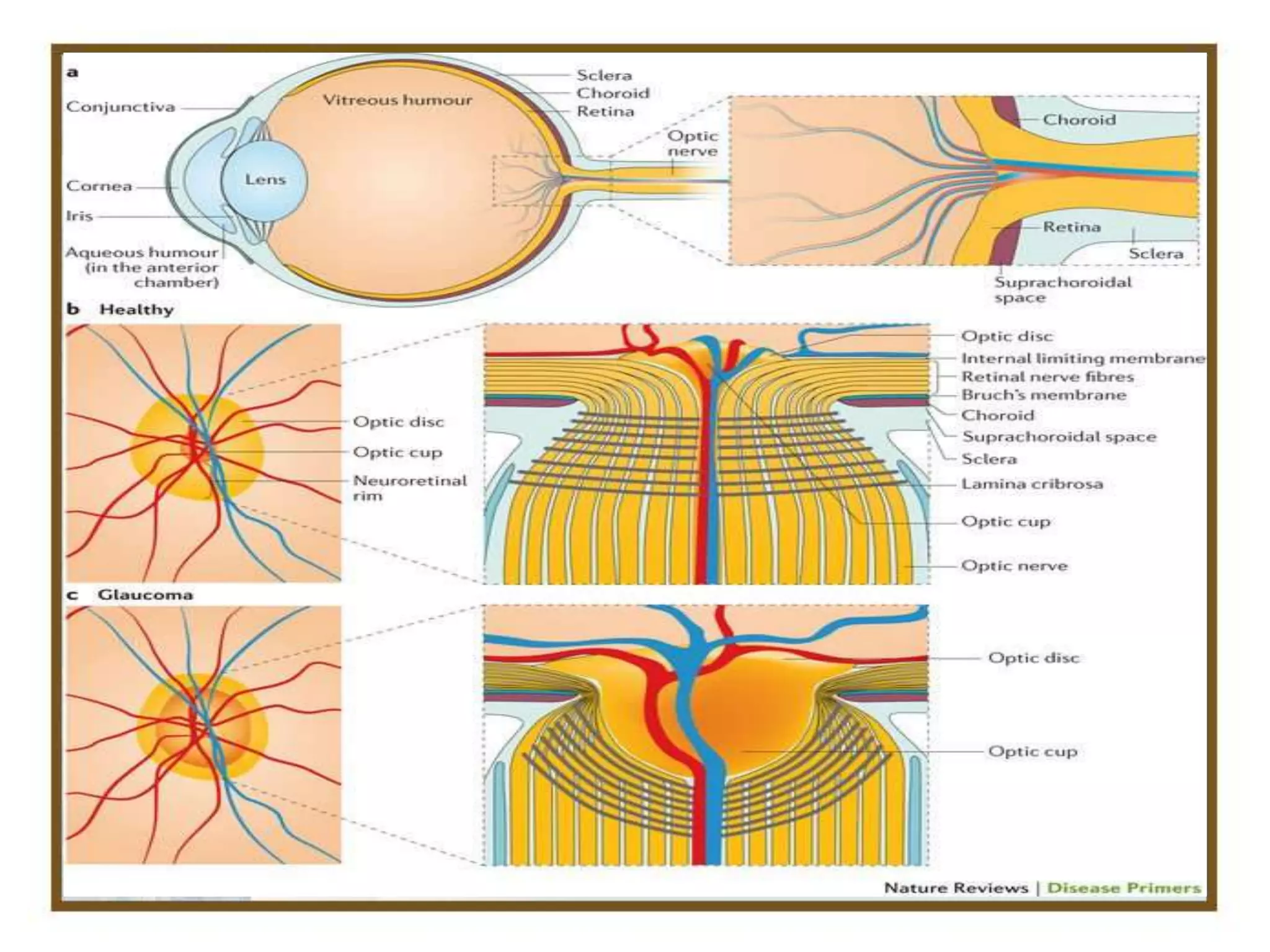
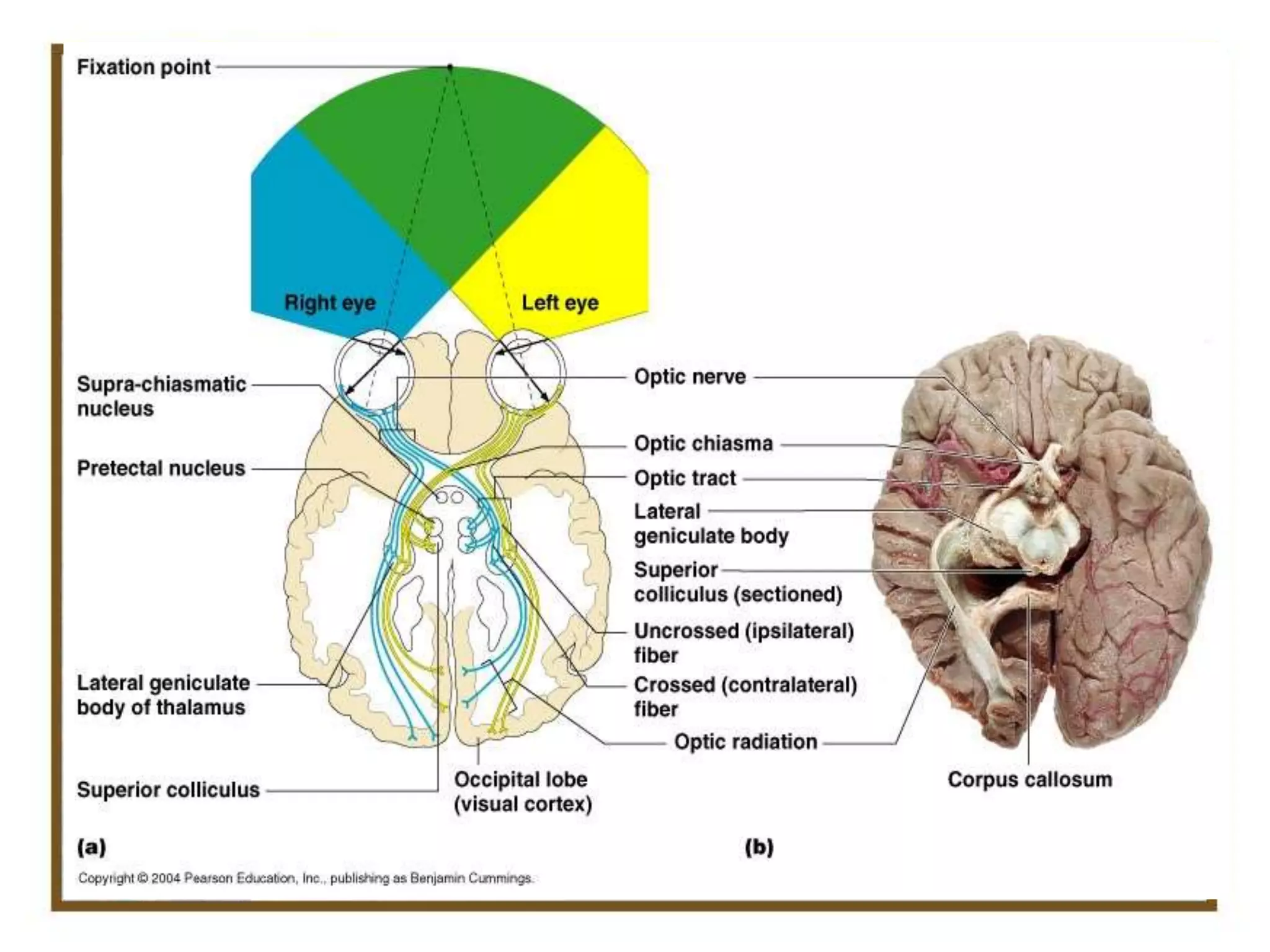
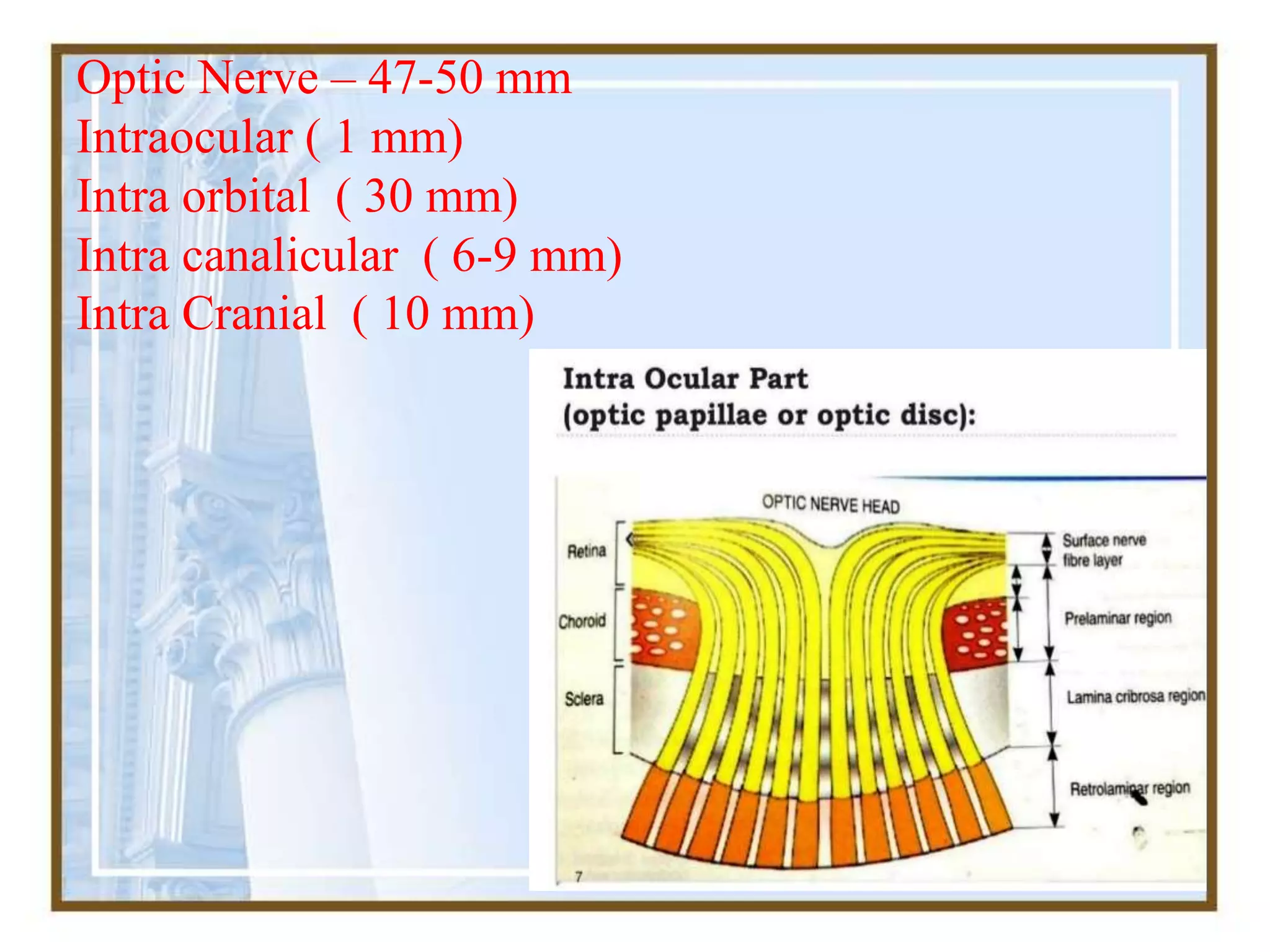
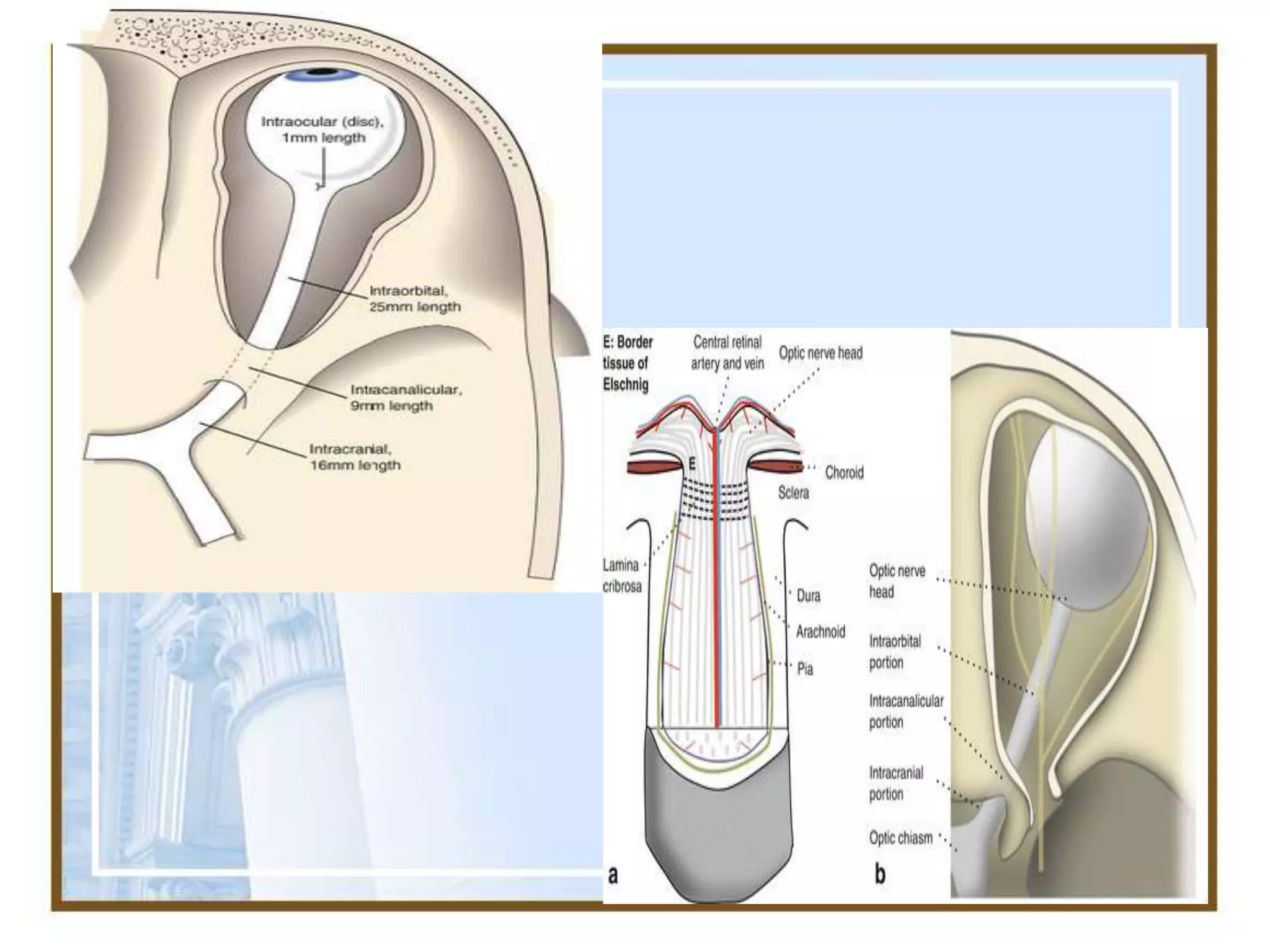
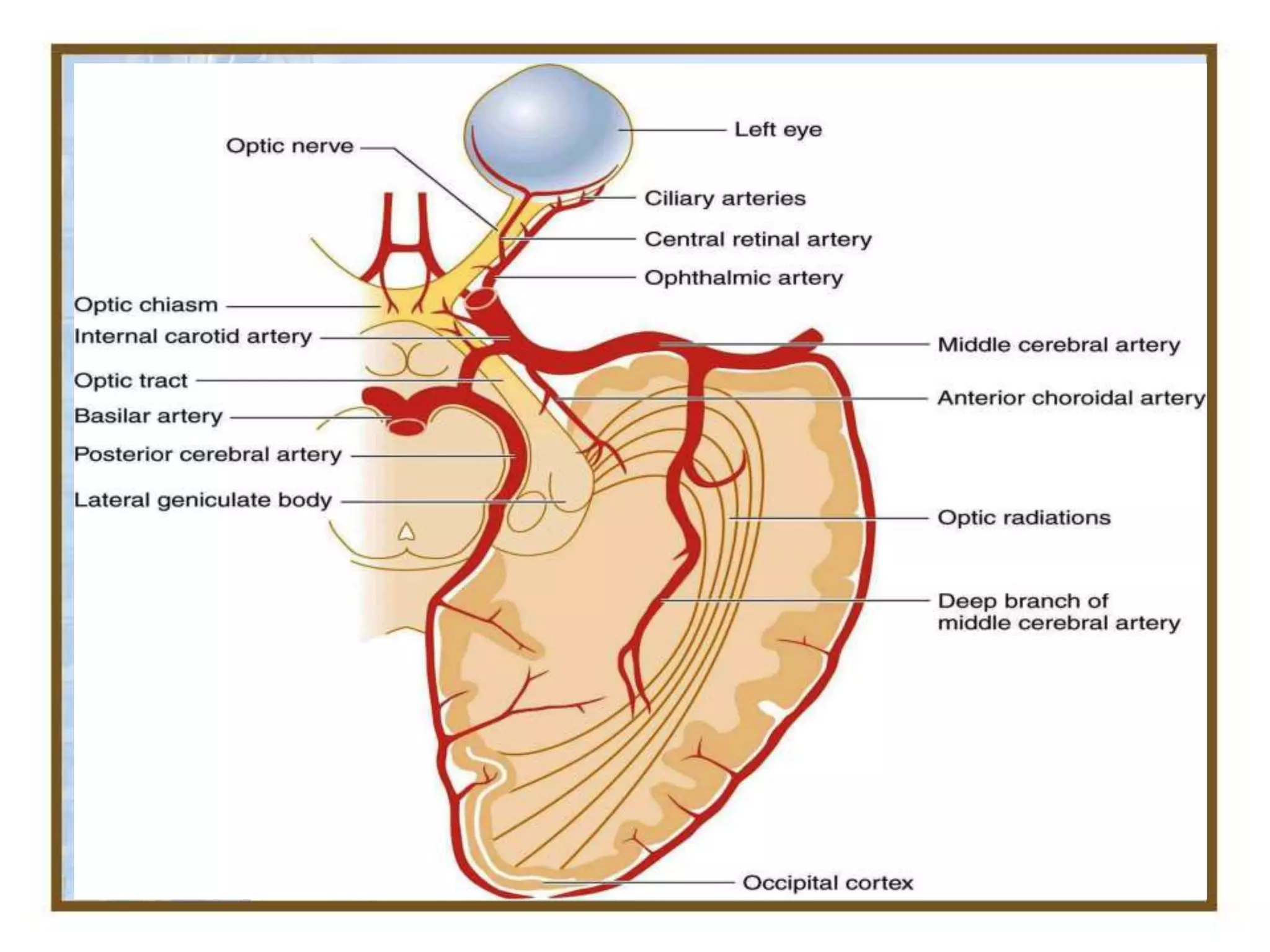
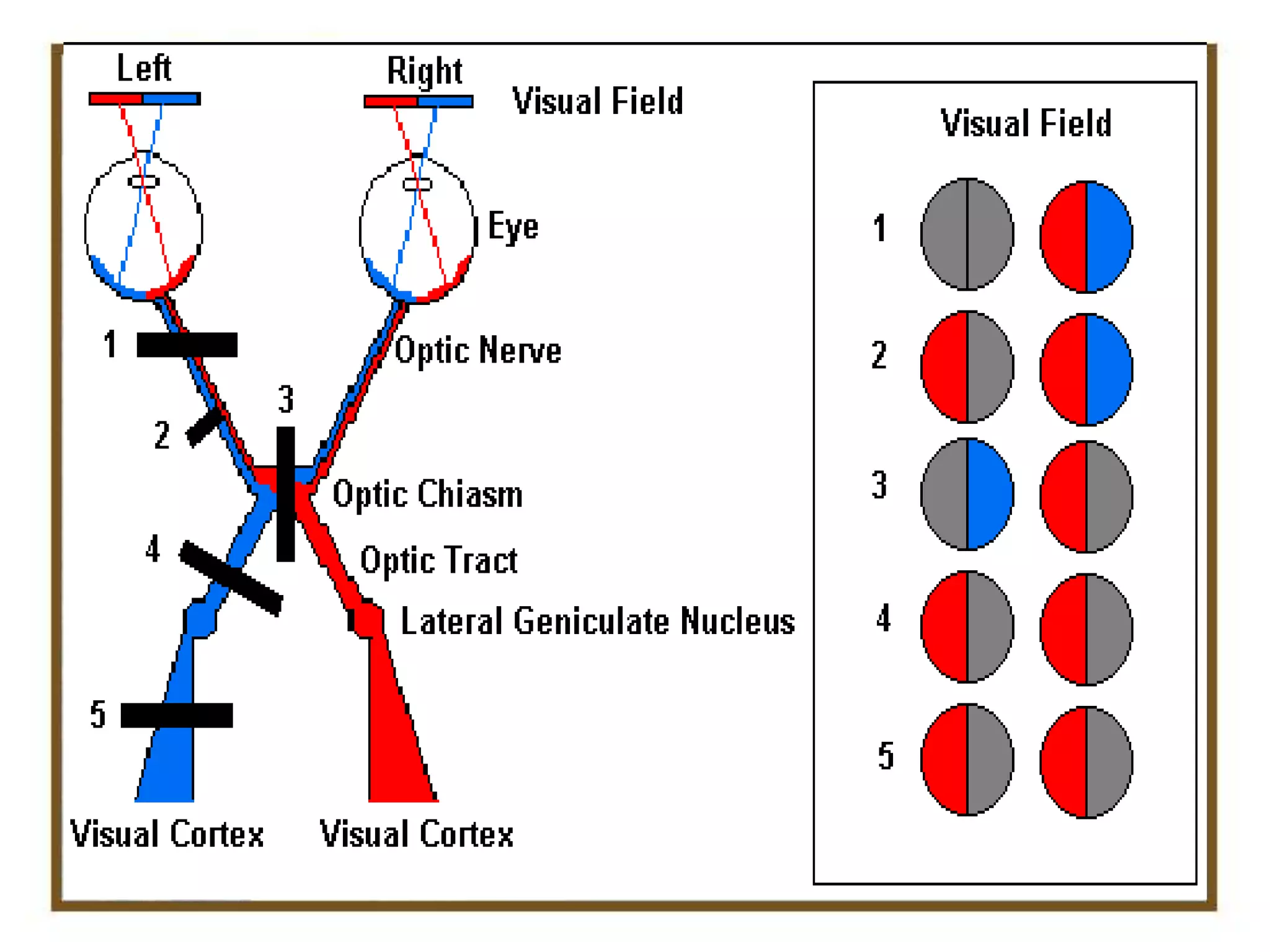
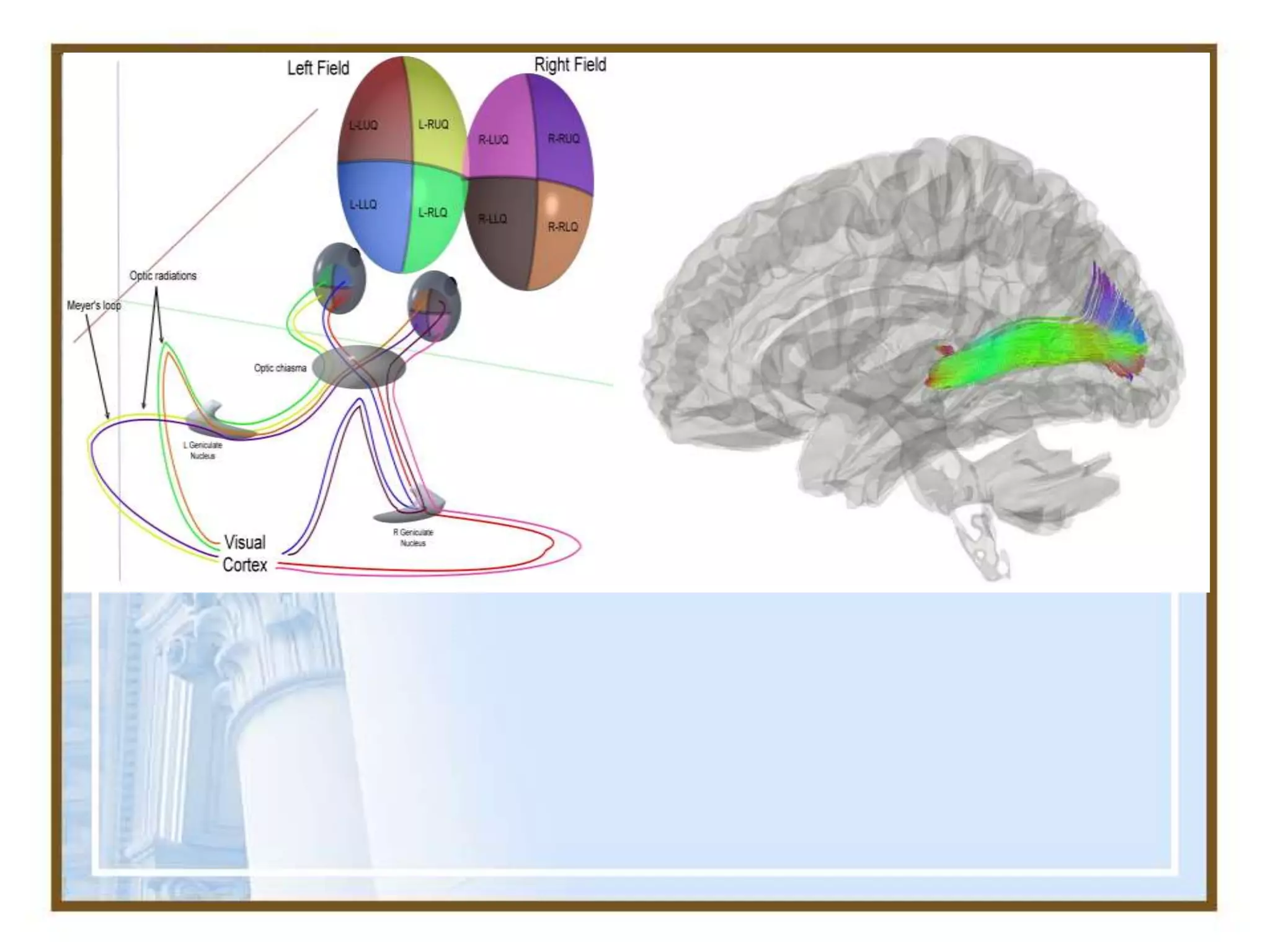
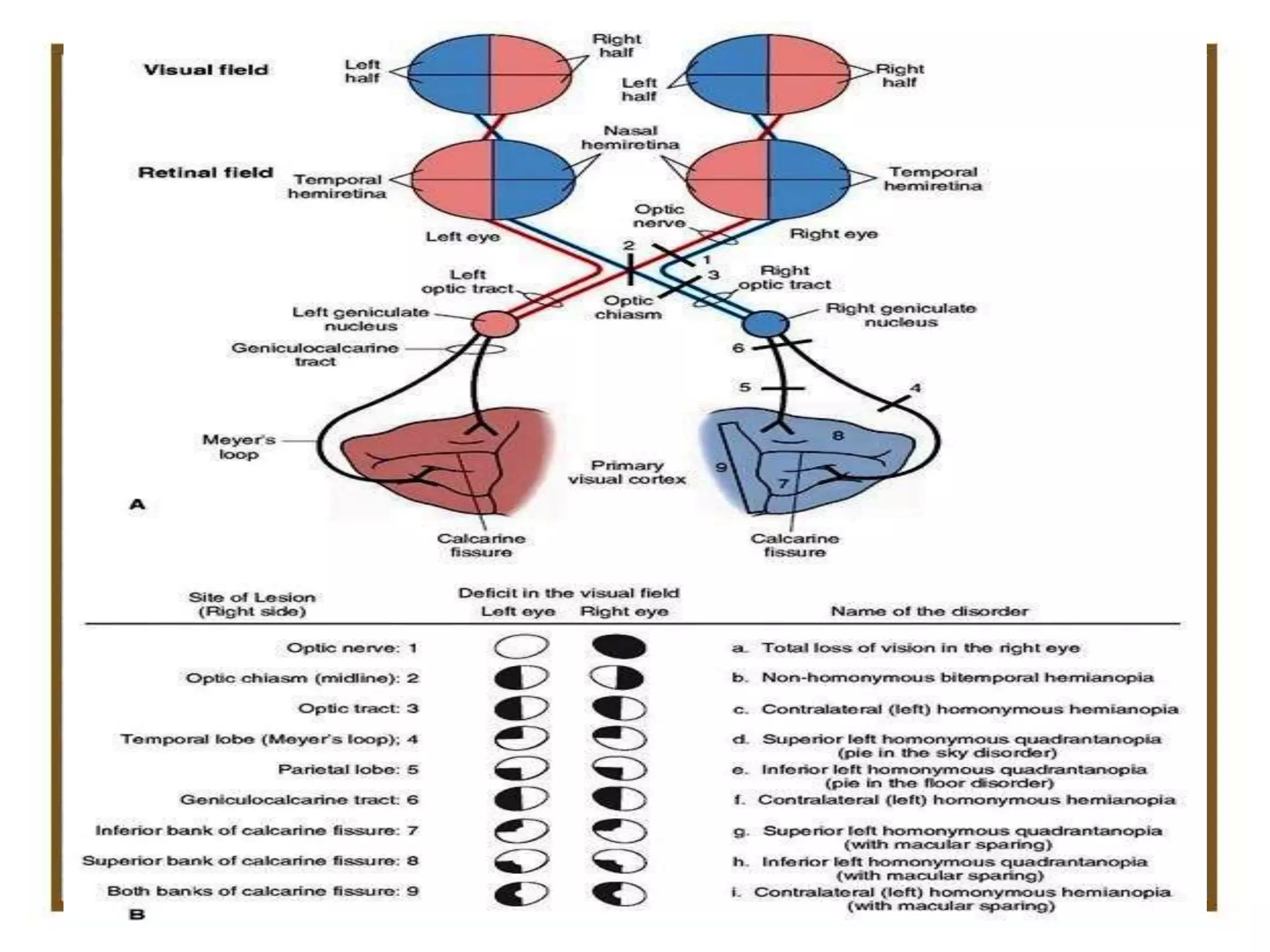
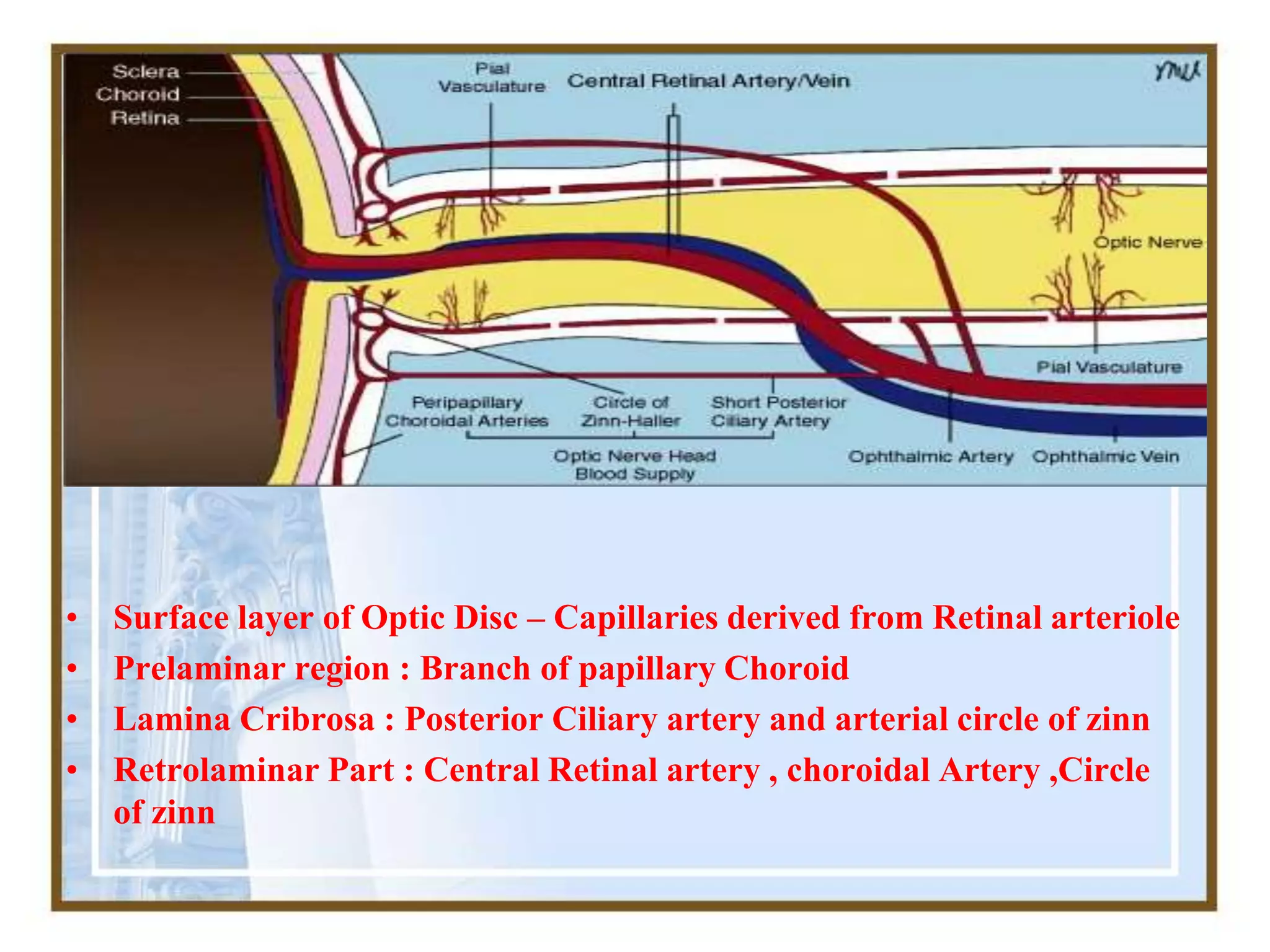
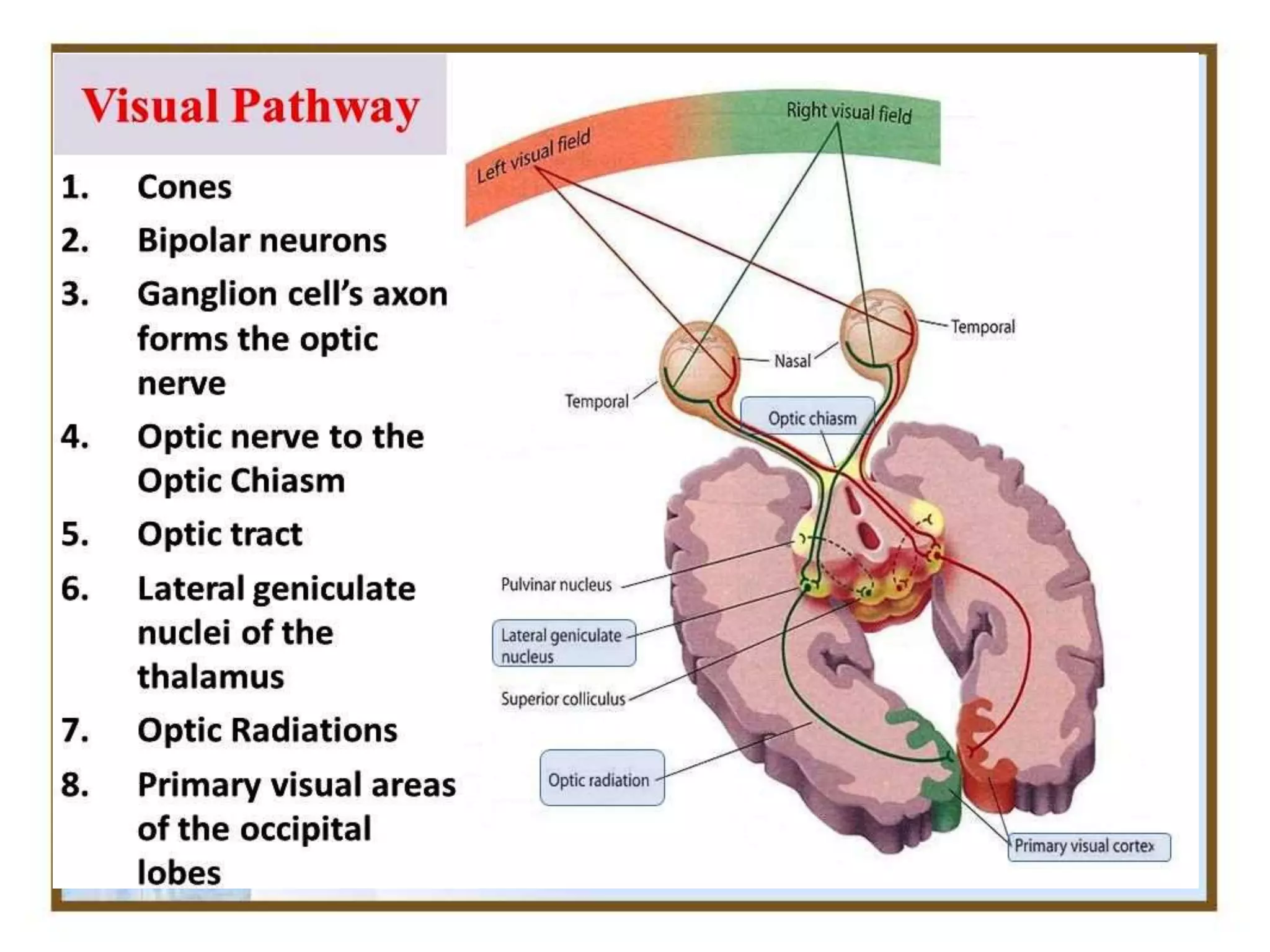
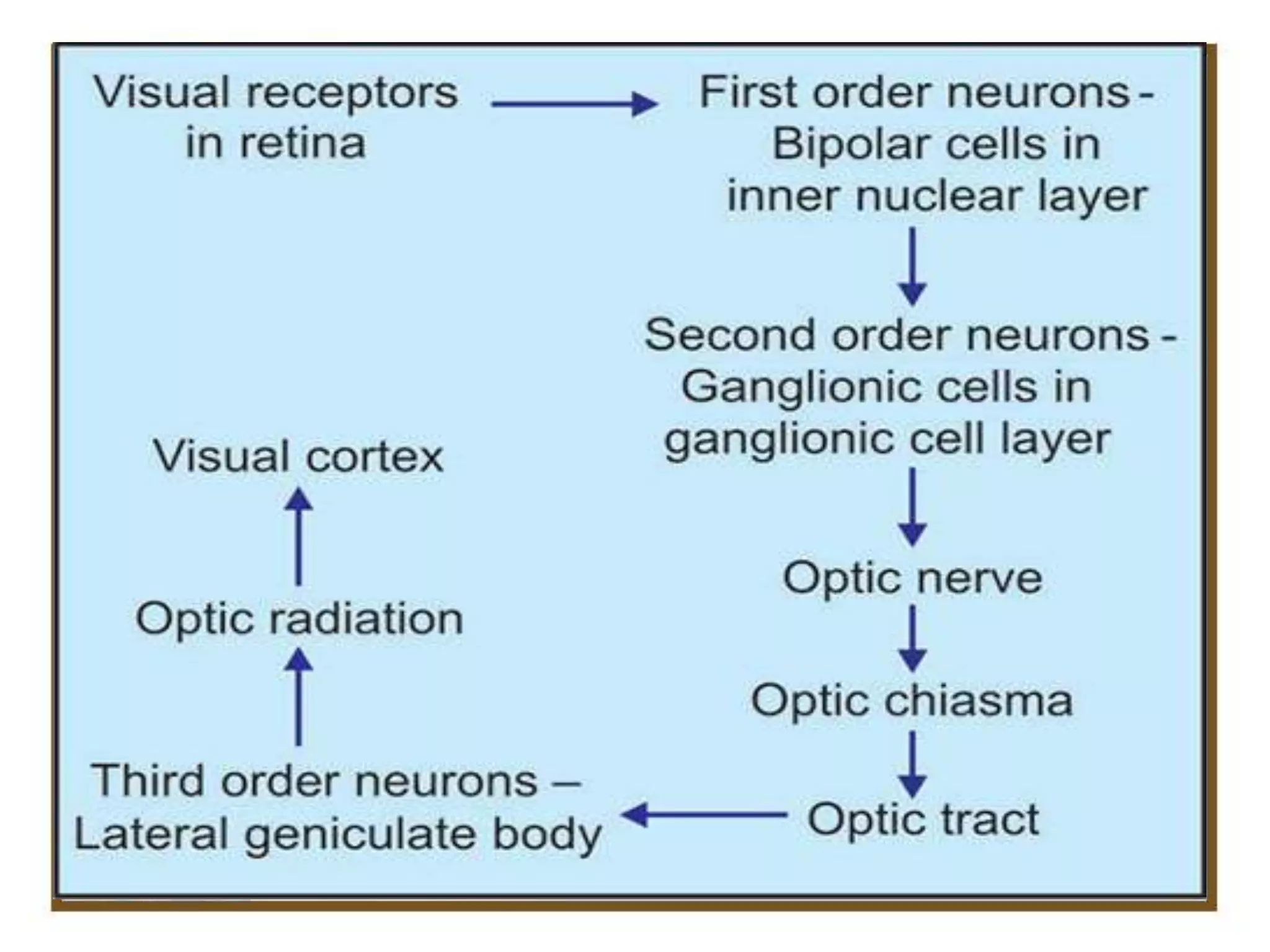
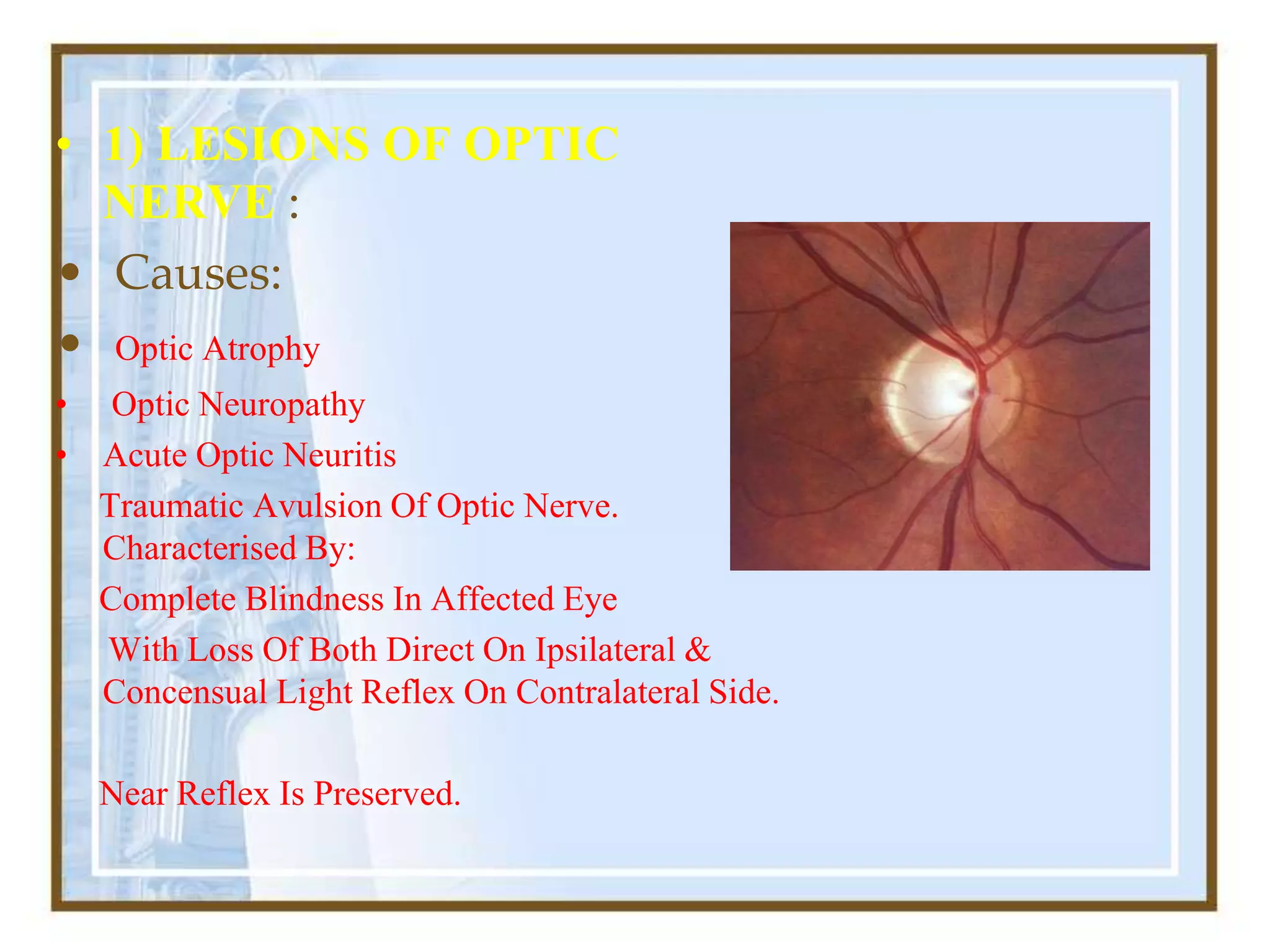
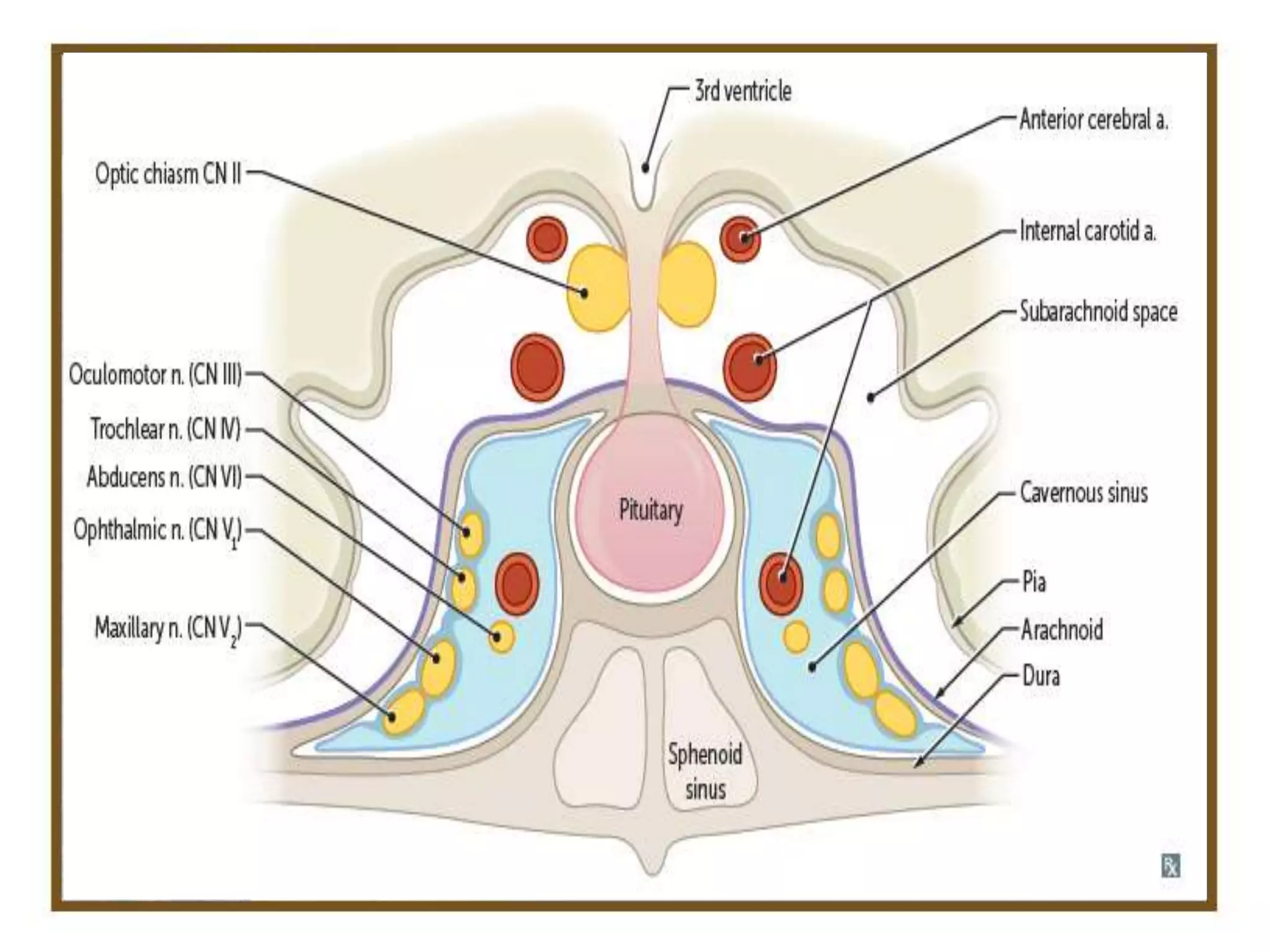
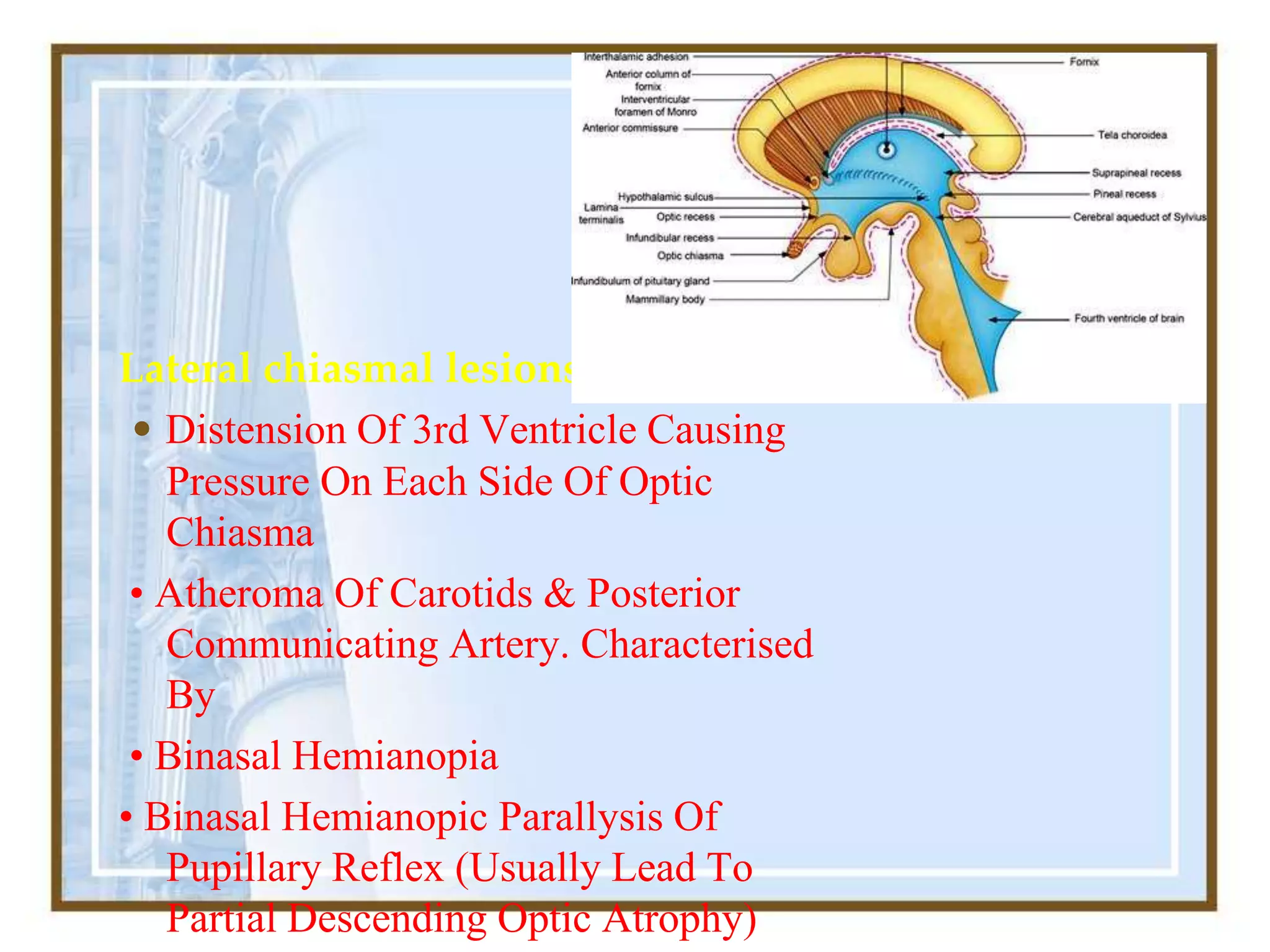
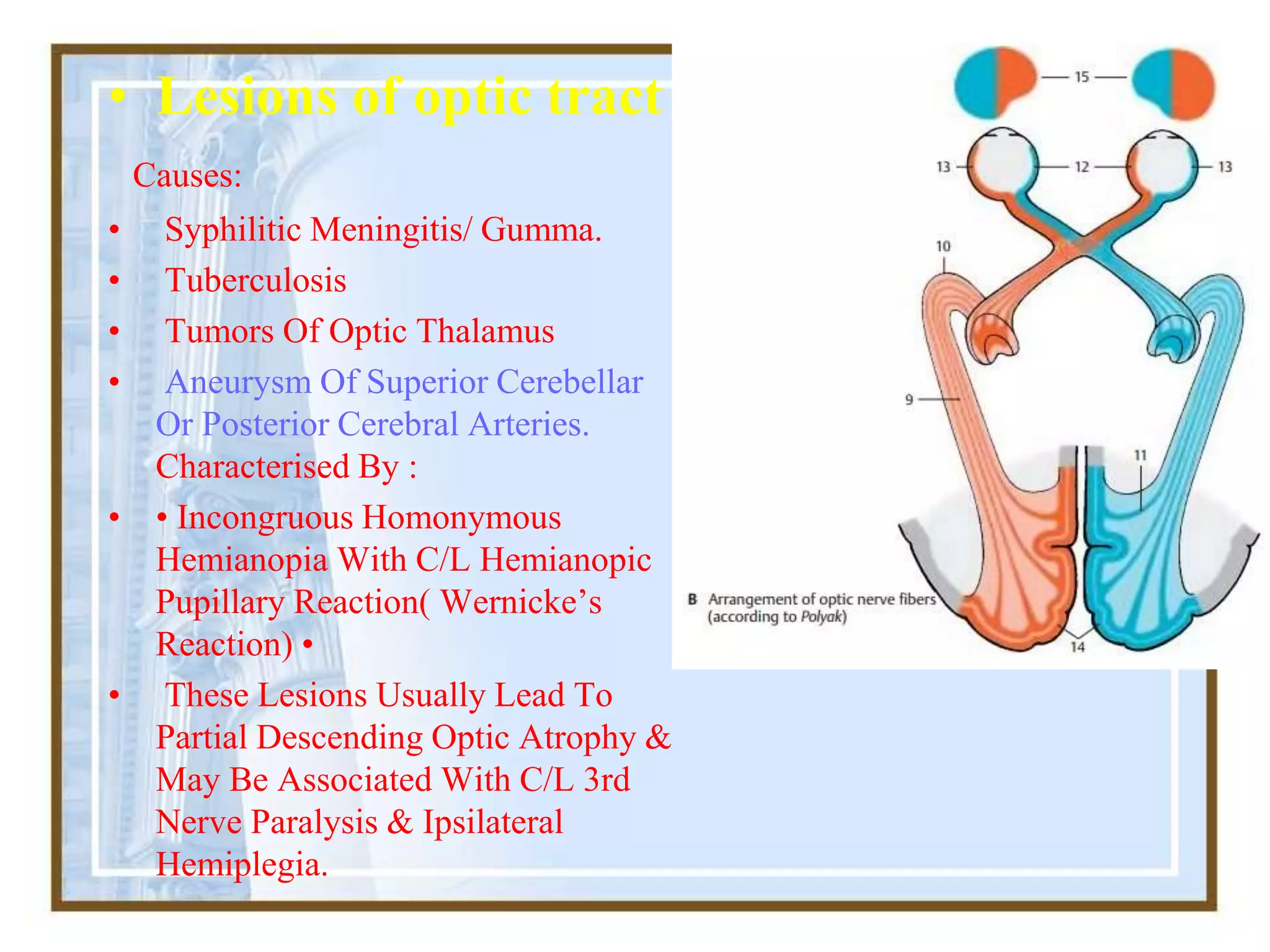
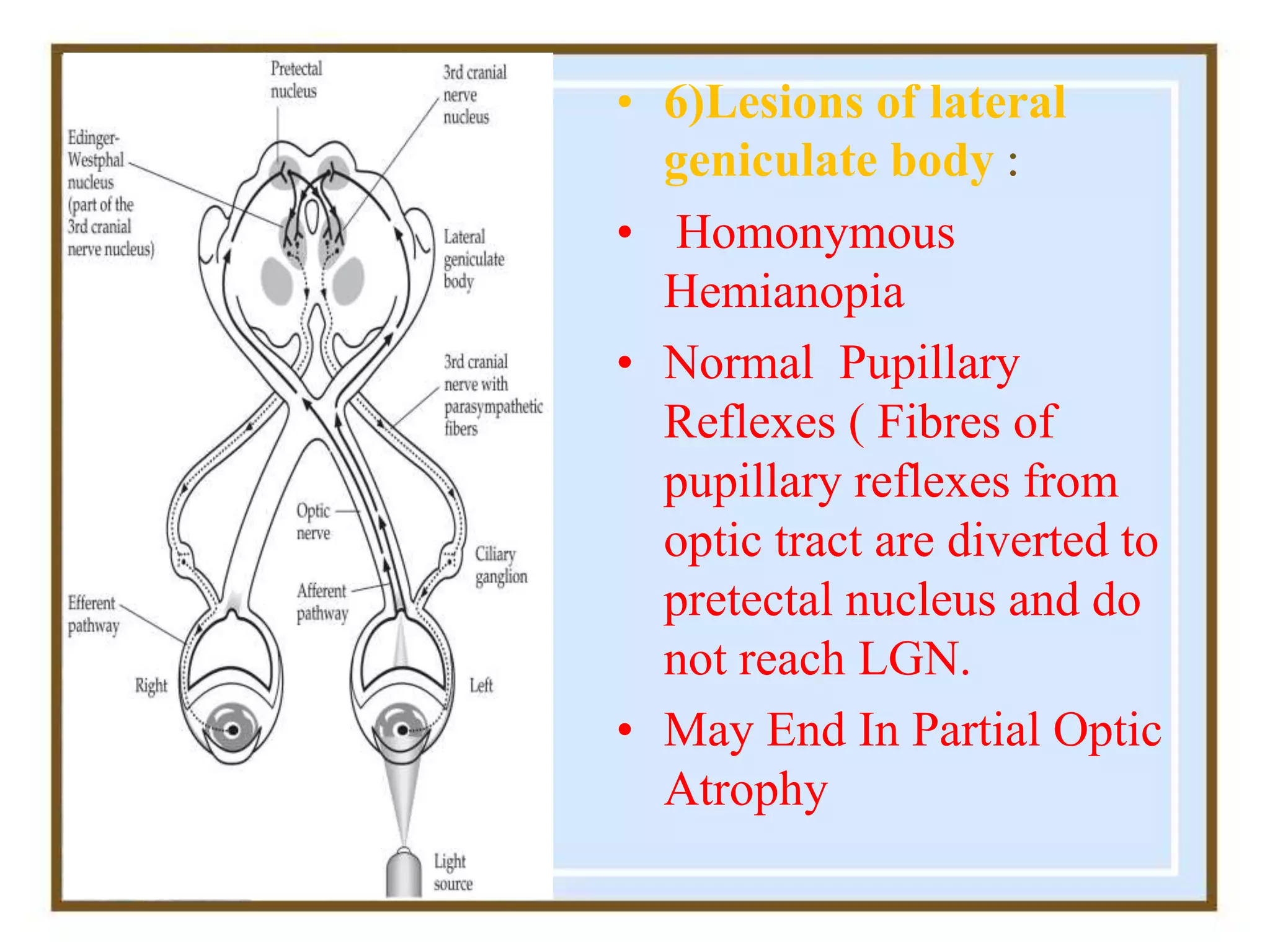
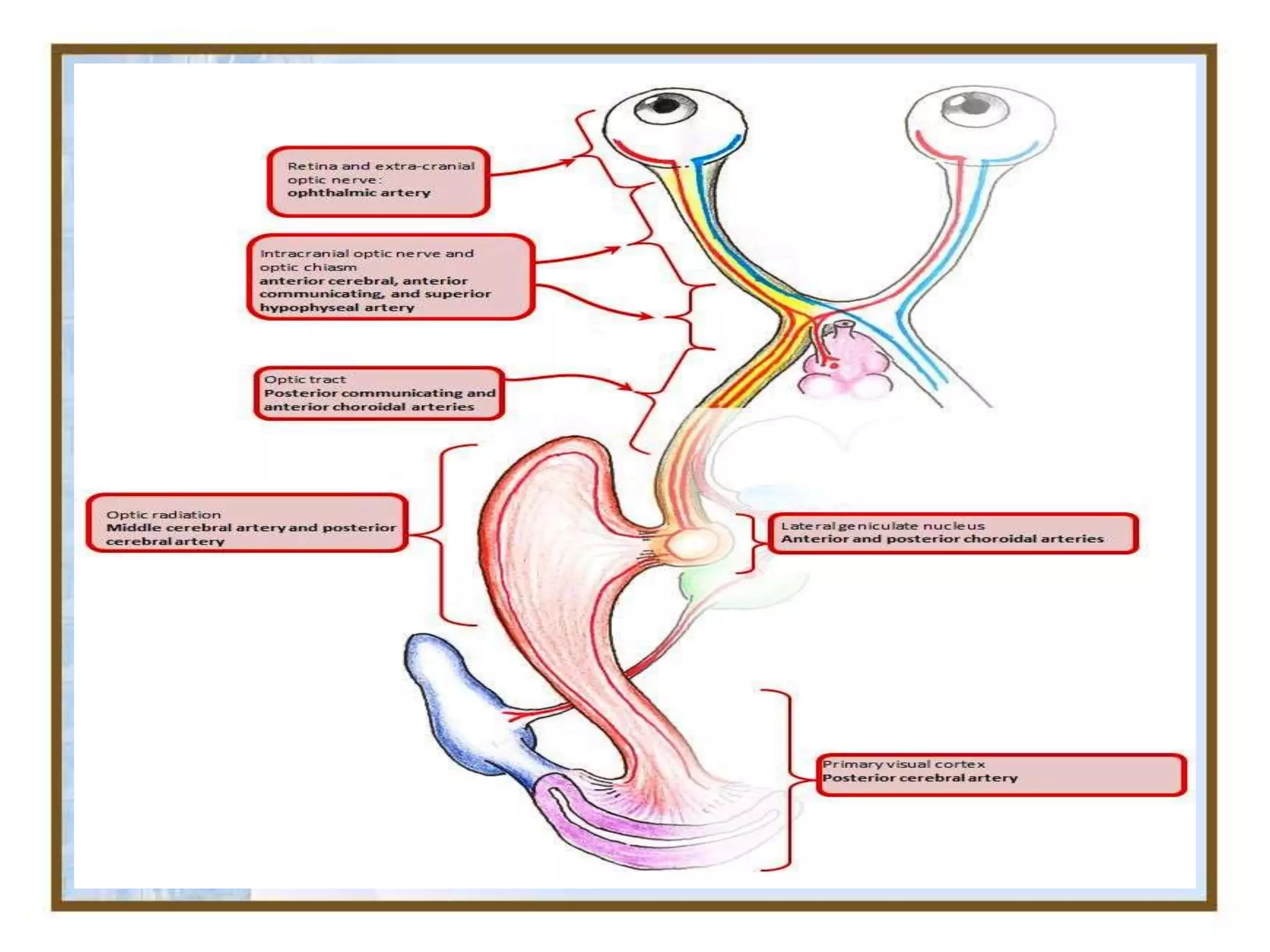
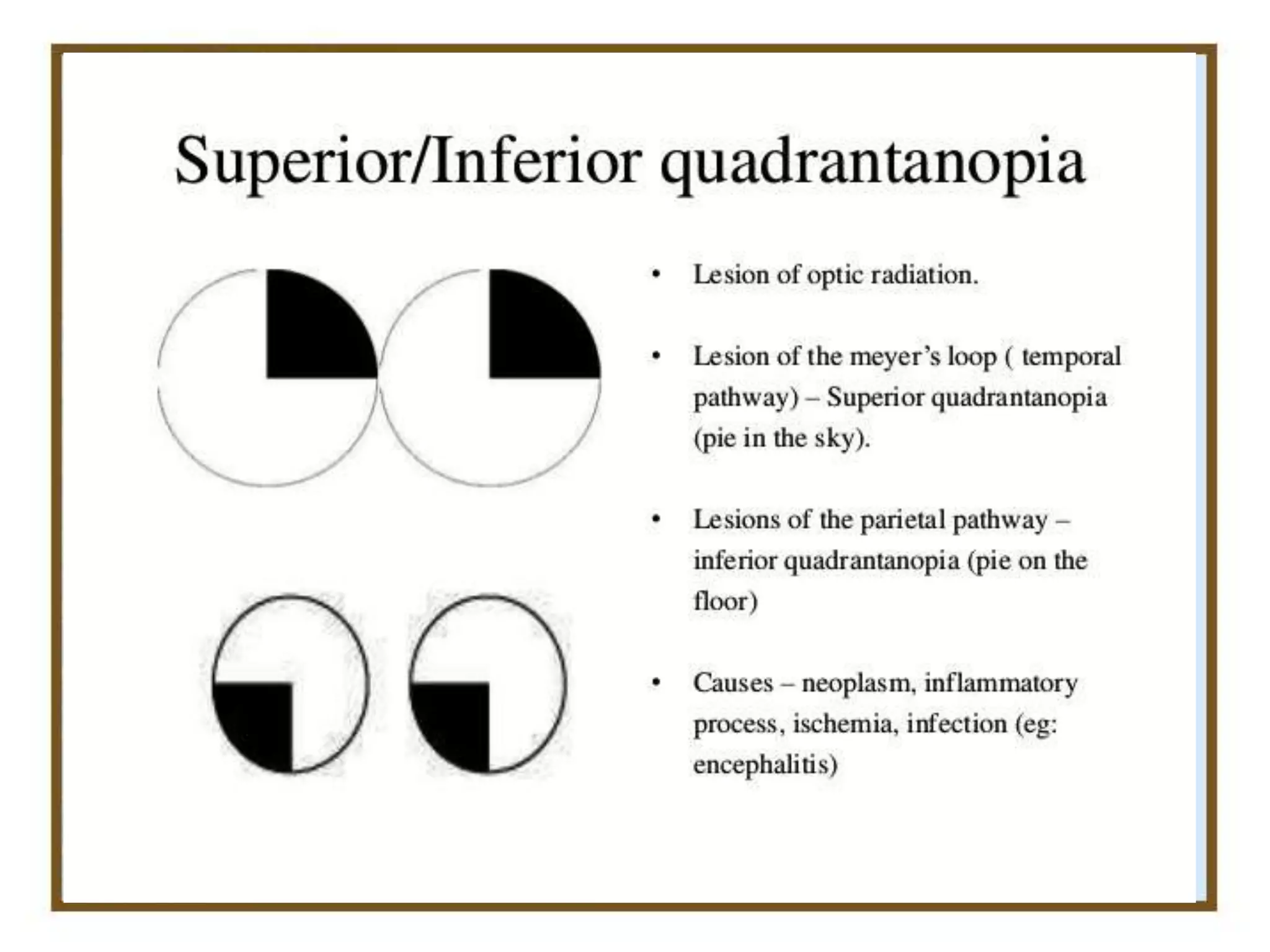
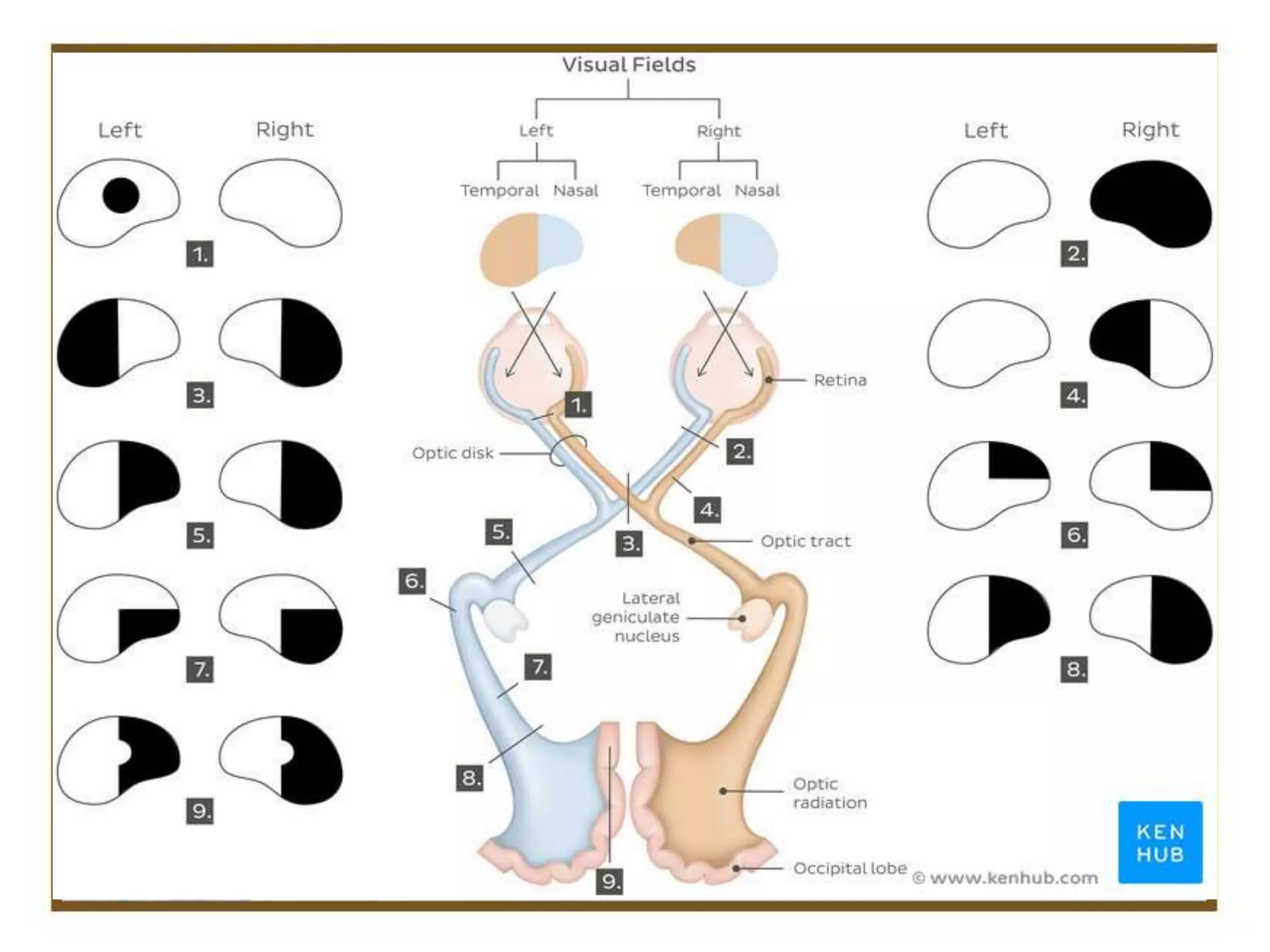
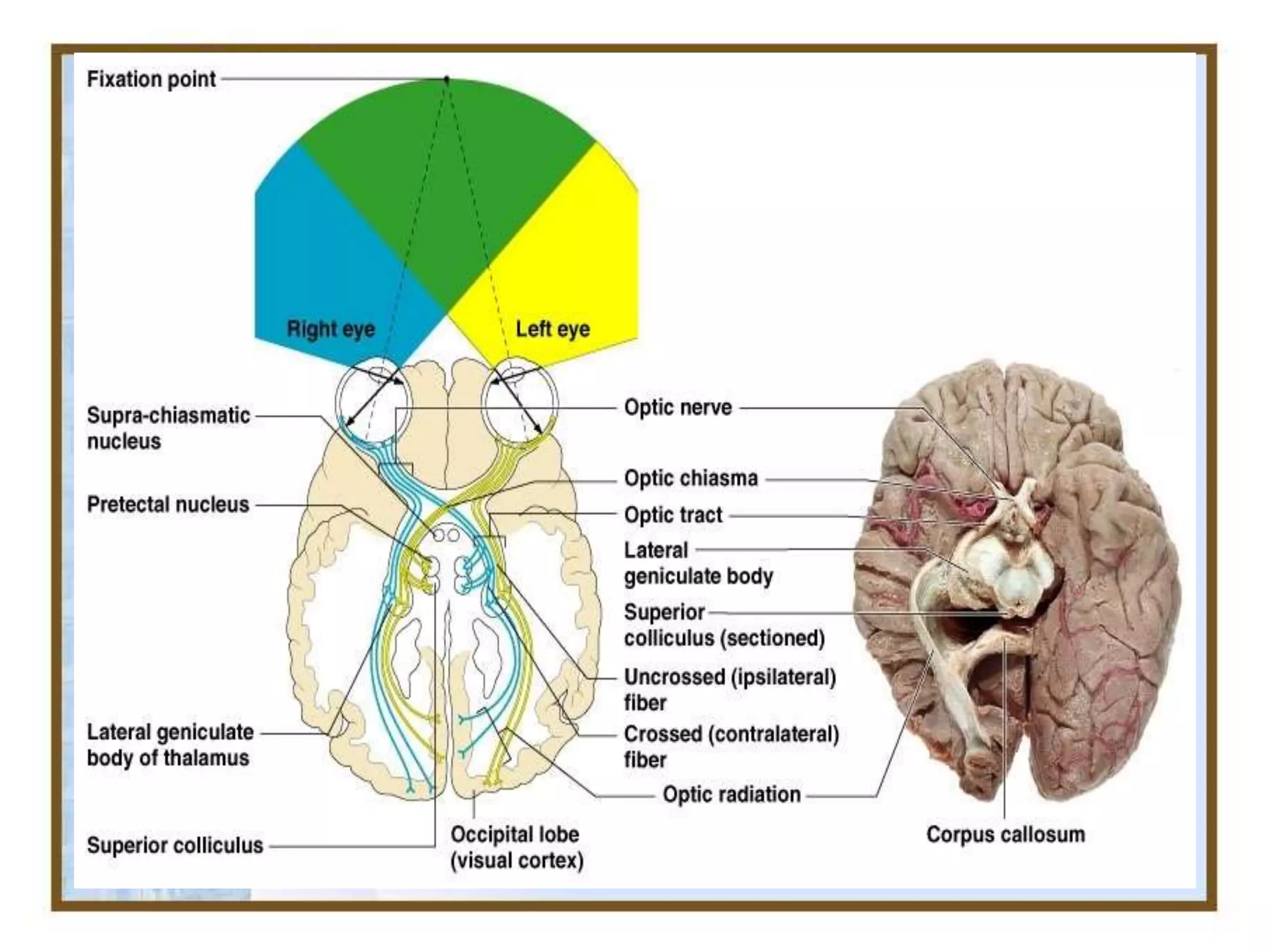


The document provides information about the optic nerve and visual pathway, including: 1. It describes the anatomy of the optic nerve from the retina through the optic chiasm and optic tracts to the visual cortex. 2. It discusses common lesions that can occur at different points along the visual pathway and their associated visual field defects. 3. It outlines the blood supply and venous drainage of the optic nerve and visual pathway structures.























































































