Downloaded 1,855 times
![Causes for central scotoma
Demylineation[retrobulbar neuritis]
Leber’s hereditary optic neuropathy
Toxins-
tobacco,lead,alcohol,methanol
Vitamin B12 deficiency](https://image.slidesharecdn.com/visualpathway-120825075100-phpapp01/85/Visual-pathway-21-320.jpg)

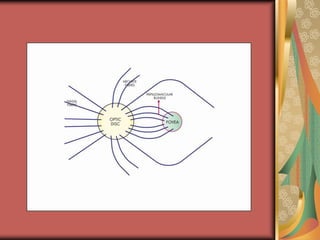
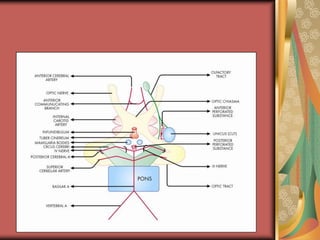
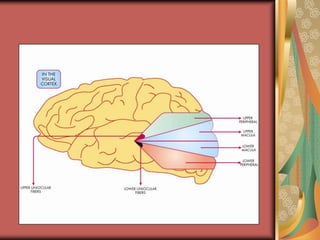
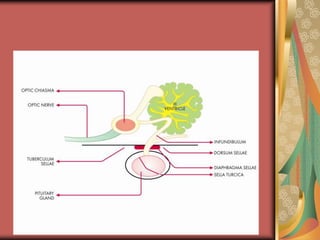
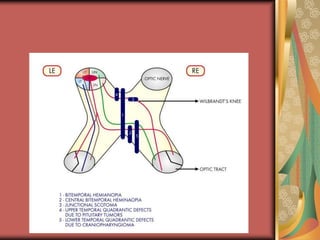
![Location of chiasma
Central fixation -80%- above the sella
Pre fixed chiasm-10%-located anteriorly-
so pitutary tumour involves the optic tract
first [lower temporal fields first]
Post fixed chiasm-10%-located posteriorly-
so optic nerve gets involved first
[upper temporal fields first]](https://image.slidesharecdn.com/visualpathway-120825075100-phpapp01/85/Visual-pathway-29-320.jpg)


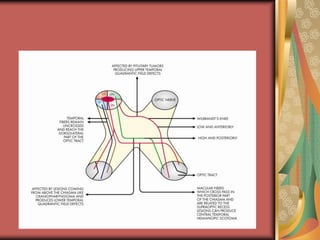
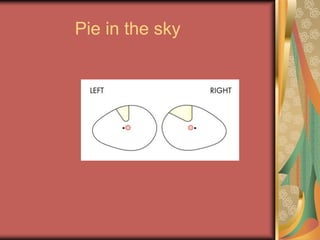
![TEMPORAL LOBE
Controlateral congruous
homonymous superior
quadrantanopia[pie in the sky]
Controlateral hemisensory
disturbance
Mild hemiparesis
Paraxysomal olfactory and uncinate
fits.
Formed visual hallucinations](https://image.slidesharecdn.com/visualpathway-120825075100-phpapp01/85/Visual-pathway-45-320.jpg)
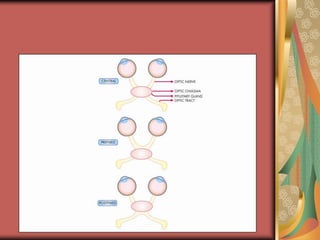
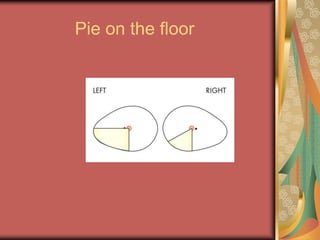
![PAREITAL LOBE
Controlateral congruous homonymous
inferior quadrantanopia[pie on the floor]
Visual perception difficulties
Right-left confusion
Acalculia
Assymmetric OKN.[OKN response
diminished towards the side of the
lesion.]](https://image.slidesharecdn.com/visualpathway-120825075100-phpapp01/85/Visual-pathway-47-320.jpg)
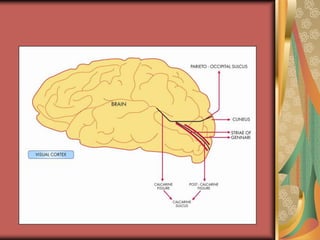
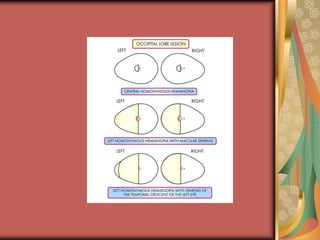
![Striate calcarine cortex
Congruous homonymous hemianopias
with macular sparing, macular
involvement alone.
Formed visual hallucinations.
Anton's syndrome[ denial of blindness]
Riddoch phenomenon](https://image.slidesharecdn.com/visualpathway-120825075100-phpapp01/85/Visual-pathway-49-320.jpg)

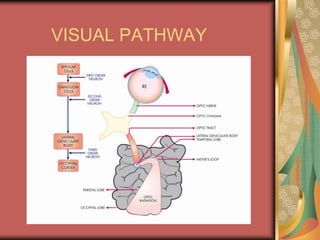
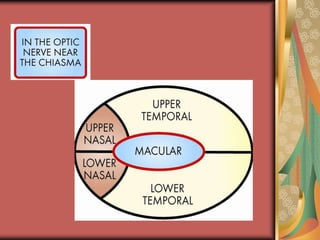
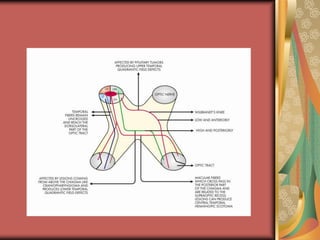
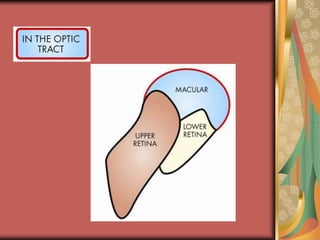
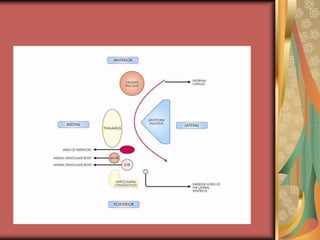
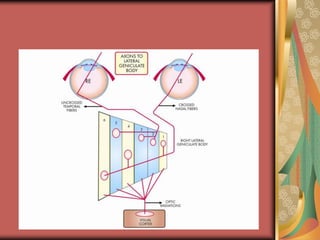
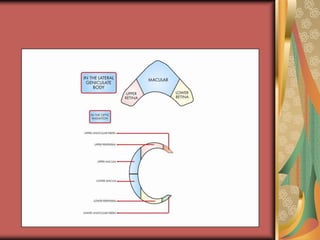
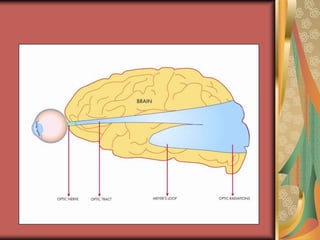
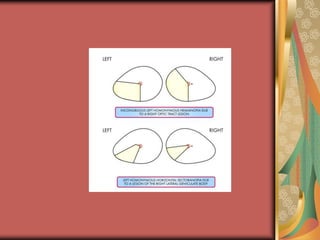
The document outlines the anatomy and pathology of the visual pathway, detailing the structure and function of the optic nerve and related visual field defects. It discusses various conditions that can lead to different types of visual field losses, such as central scotoma and hemianopia, alongside lesions in the optic nerve, optic tract, and optic radiation. The document also covers associated symptoms and the implications of optic nerve-related diseases, emphasizing the clinical features and their neurological correlations.










































































































