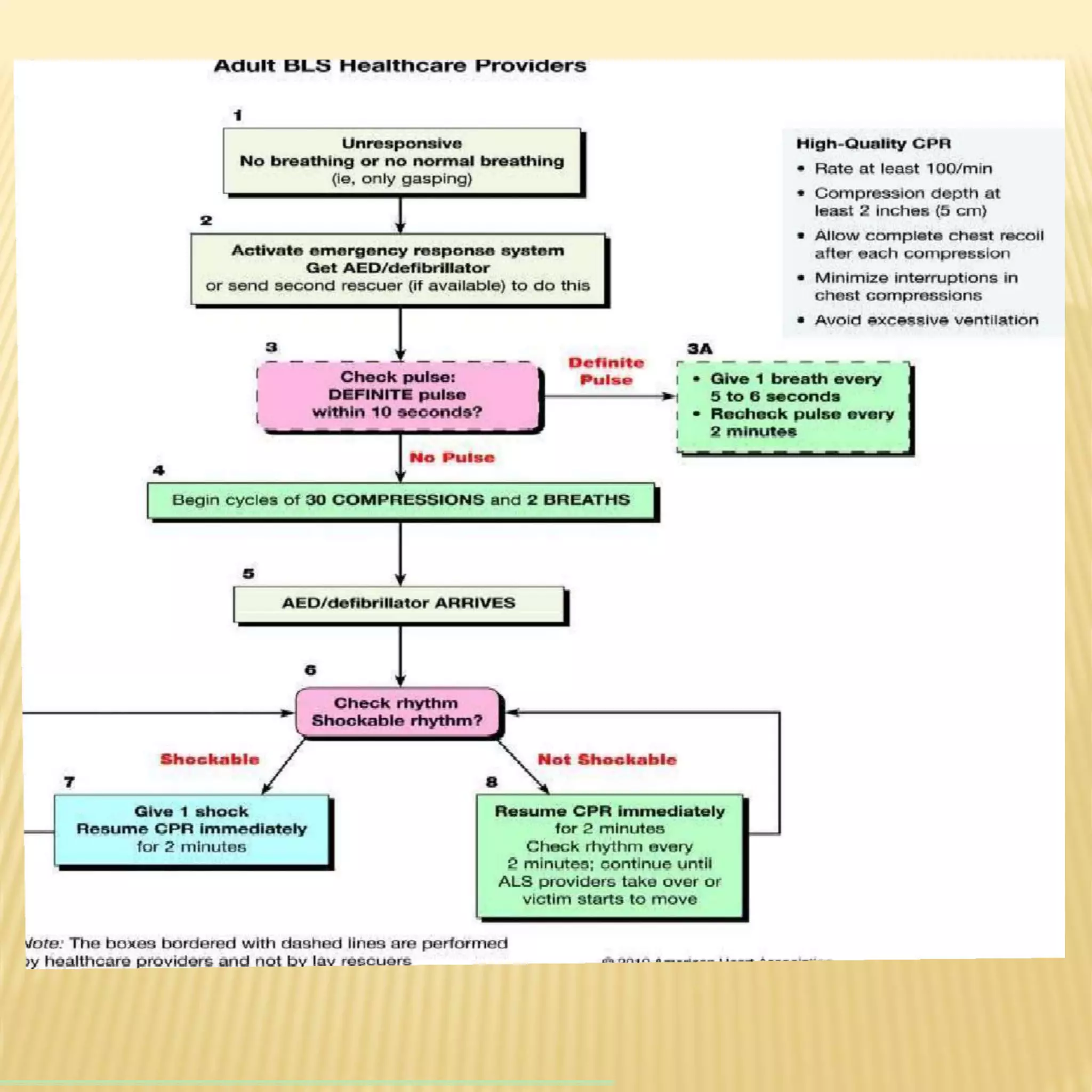
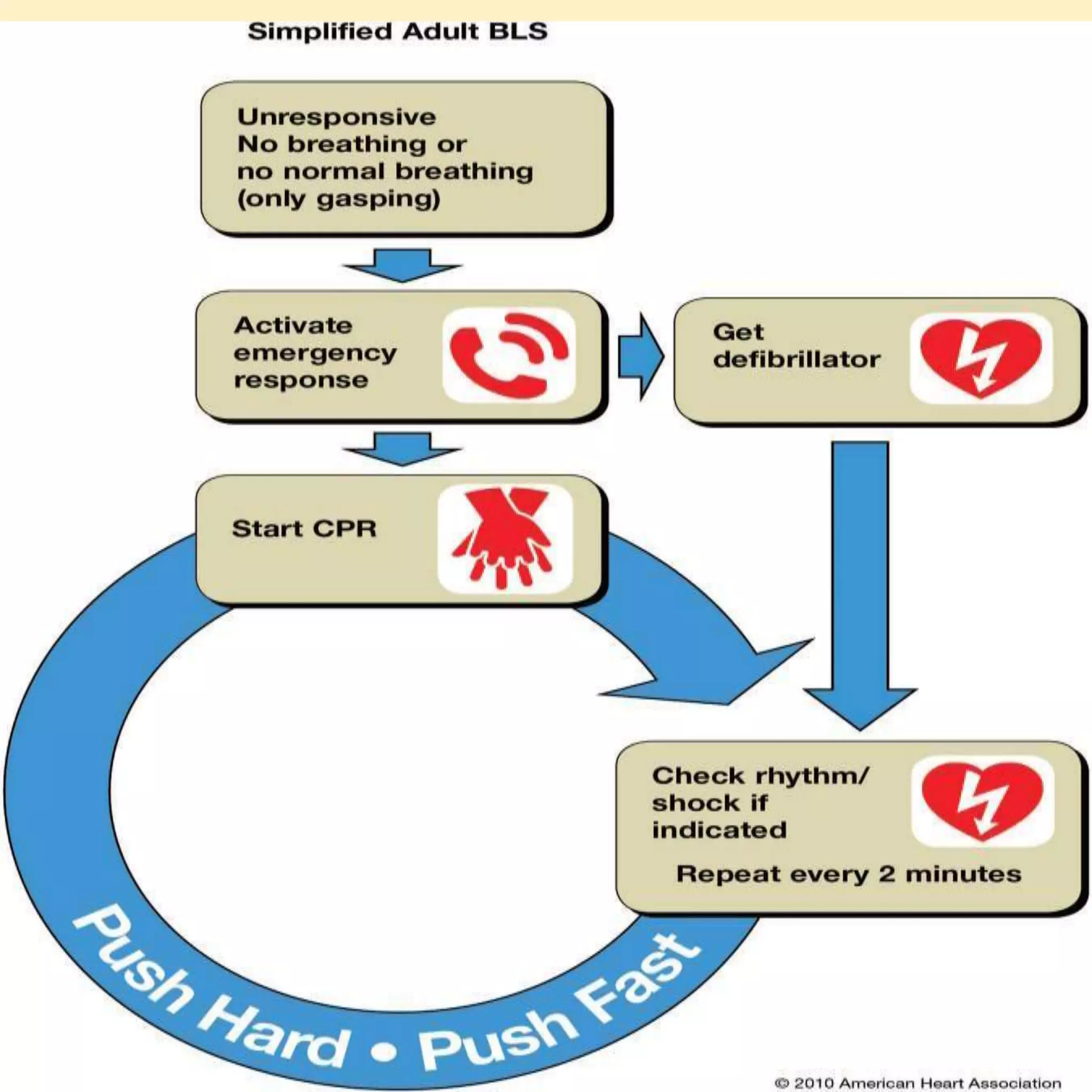
Basic life support (BLS) refers to emergency care provided to patients experiencing cardiac arrest, respiratory failure, or airway obstruction. It includes chest compressions, use of an automated external defibrillator, and relieving airway obstructions. The chain of survival emphasizes early CPR, early defibrillation, early advanced life support, and post-cardiac arrest care to maximize patient survival. BLS procedures include assessing the patient for responsiveness, activating emergency services, performing high-quality chest compressions, opening the airway, and providing rescue breaths. Defibrillation is key for shockable cardiac rhythms like ventricular fibrillation. BLS aims to provide oxygenated blood flow to vital organs until further medical help







![ENSURE SAFETY
13
Safety Of Self
Safety Of Patient
Movement of a trauma victim – only when
absolutely necessary
[unstable cervical spine – injured spinal cord]](https://image.slidesharecdn.com/basiclifesupport2021bls-210808030956/75/Basic-life-support-2021-bls-13-2048.jpg)