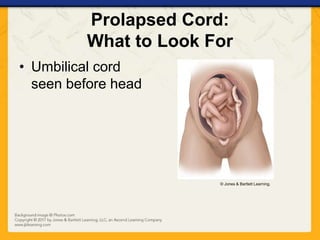
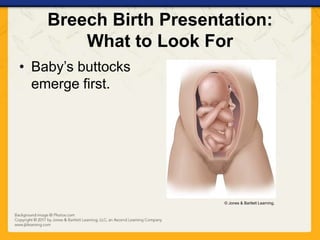
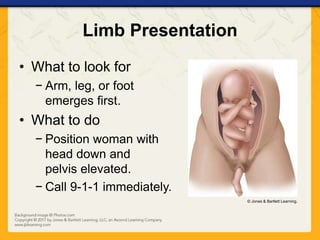
This document discusses childbirth and gynecologic emergencies. It covers topics like the signs and symptoms of miscarriage, vaginal bleeding during pregnancy, emergency delivery procedures, stages of labor, and complications during delivery such as breech birth or prolapsed umbilical cord. It also discusses the initial care of the newborn and gynecologic emergencies in nonpregnant women including sexual assault and rape.

















































































![Hypothalamus short notes on location, function and disorders by Dr. Neha [PT]...](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124142231-2b48143d-thumbnail.jpg?width=640&height=640&fit=bounds)

















