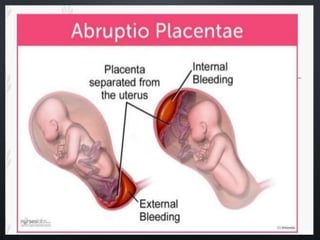
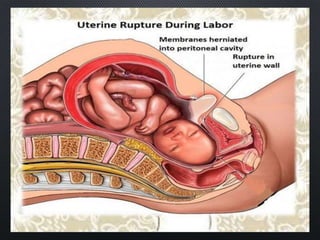
Obstetrical emergencies are life-threatening medical conditions that occur in pregnancy, during labor and delivery, or after childbirth. They can endanger the health and lives of both the mother and baby. Common obstetric emergencies include ectopic pregnancy, placental abruption, preeclampsia, premature rupture of membranes, uterine inversion or rupture, prolapsed umbilical cord, shoulder dystocia, and postpartum hemorrhage. Diagnosis involves medical history, examination, and tests, while treatment depends on the specific emergency but may include bed rest, medications, premature delivery by c-section or other surgery, or hysterectomy in severe cases.
















































![maternal guide presentation [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/maternalpresentationautosaved-250208125838-a01bbc1b-thumbnail.jpg?width=640&height=640&fit=bounds)

















































