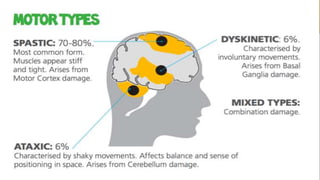
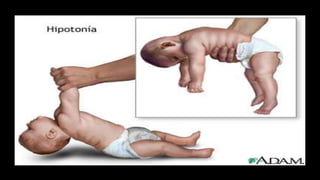
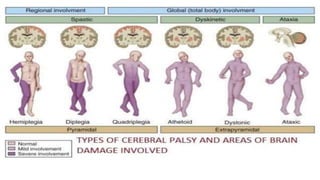
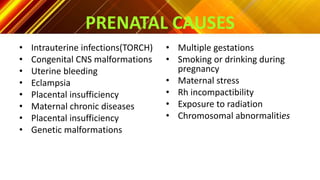
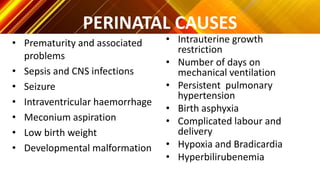
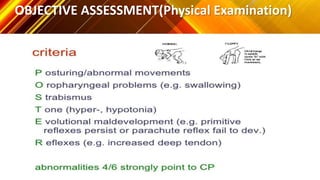
Cerebral palsy (CP) is a group of disorders that affect movement and posture as a result of damage to the developing brain. It was first described in the 1860s and can be caused by prenatal, perinatal, or postnatal factors that damage the brain such as infection, trauma, or lack of oxygen. The main types of CP are spastic, dyskinetic, ataxic, and hypotonic. Treatment involves medical management of symptoms, surgery to improve mobility, and rehabilitative therapies like physical, occupational, and speech therapy.




























































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)








