Downloaded 6,603 times
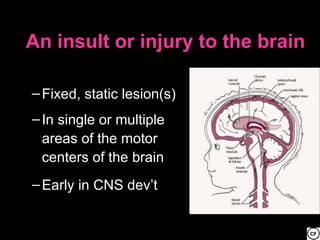
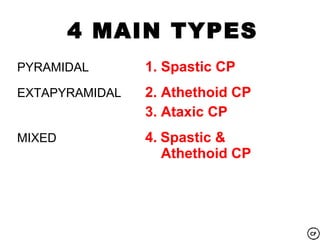
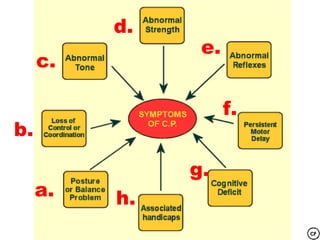





This document provides information about cerebral palsy (CP), including: 1. CP is a motor function disorder caused by permanent, non-progressive brain lesions present at birth or shortly after. It causes a lack of muscle control and balance issues. 2. CP has various causes like developmental malformations, neurological damage before/during/after birth from issues like lack of oxygen. 3. There are four main types of CP defined by affected movements: spastic, athetoid, ataxic, and mixed. Spastic CP is the most common. 4. Treatment aims to improve motor skills and independence through therapies, surgeries, medications, assistive devices, and family support













































![CP-1[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cp-11-240131015513-63dc9ac0-thumbnail.jpg?width=640&height=640&fit=bounds)
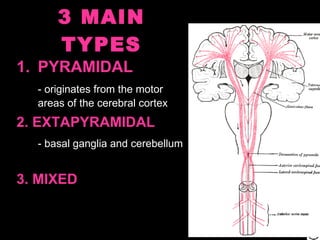
![cerebral palsy[1].pptxcerebral palsy management etiopathogenesis](https://cdn.slidesharecdn.com/ss_thumbnails/cerebralpalsy1-251219125140-a80c6a48-thumbnail.jpg?width=640&height=640&fit=bounds)


























