OCCLUSION IN FIXED
PARTIALDENTURE
Dr Athira K Nair
IIIrd
Year MDS
Department Of Prosthodontics, Crown And
Bridge
BVP Dental College, Pune
Date: 21/12/2023
2.
INDEX
• INTRODUCTION
• HISTORY
•OCCLUSION
• IMPORTANCE OF OCCLUSION
• DAWSON’S CLASSIFICATION OF OCCLUSION
• DETERMINANTS OF OCCLUSION
• CONCEPTS OF OCCLUSION
• OCCLUSAL INTERFERNCE
• PATHOLOGIC OCCLUSION
• OCCLUSAL TREATMENT
• CONCLUSION
• REFERENCES
3.
INTRODUCTION
• The stomatognathicsystem is so well architected naturally that even a
micron difference in the occlusal surface of a small restoration can be
identified by patients and cause them discomfort in functioning.
• The tissues and functions of the masticatory system are subjected to
adaptation, abuse, wear, ageing and disease.
• Occlusion, is, therefore, a changing condition and the responses to
change vary between healthy adaptation and total disorder.
4.
DEFINITIONS
OCCLUSION
MAXIMUM INTERCUSPATION
The staticrelationship between the incising or masticating surfaces of the maxillary or
mandibular teeth or tooth analogues
The complete intercuspation of theopposing teeth independent of condylar position, sometimes
referred to as the best fit of the teeth regardless of the condylar position.
The glossary of prosthodontics terms. J Prosthet Dent
5.
CENTRIC RELATION
CENTRIC OCCLUSION
Amaxillomandibular relationship, independent of tooth contact, in which the condyles
articulate in the anterior-superior position against the posterior slopes of the articular
eminences; in this position, the mandible is restricted to a purely rotary movement; from this
unstrained, physiologic,maxillomandibular relationship, the patient can make vertical, lateral
or protrusive movements; it is a clinically useful, repeatable reference position
The occlusion of opposing teeth when the mandible is in centric relation; this may or may not
coincide with the maximal intercuspal position
The glossary of prosthodontics terms. J Prosthet Dent
6.
ANTERIOR GUIDANCE
CONDYLAR GUIDANCE
Theinfluence of the contacting surfaces of anterior teeth, limiting mandibular movements
Mandibular guidance generated by the condyle and articular disc traversing the contour of the
articular eminence.
The glossary of prosthodontics terms. J Prosthet Dent
7.
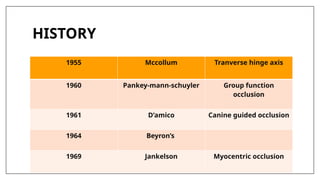
HISTORY
1955 Mccollum Tranversehinge axis
1960 Pankey-mann-schuyler Group function
occlusion
1961 D’amico Canine guided occlusion
1964 Beyron’s
1969 Jankelson Myocentric occlusion
8.
OCCLUSION
Ideal occlusion canbe defined as an occlusion which is compatible
with stomatognathic system providing efficient mastication and
good esthetics without creating physiologic abnormalities.
-
HOBO, 1978
9.
DAWSON (1974) alsohas put forth his ideas for deriving an ideal
occlusion
1. Stable stops on all teeth when the condyles are in the most superior
posterior position.
2. An anterior guidance that is harmony with the border movements of
the envelop of function.
3. Disocclusion of all the posterior teeth in protrusive movements.
4. Disocclusion of all posterior teeth on the balancing side.
5. Non interference of all posterior teeth on the working side with either
the lateral anterior guidance or the border movements of the
condyles
10.
IMPORTANCE OF OCCLUSION
Patient comfort
Reduce head aches
Rectify periodontal disease and TMJ dysfunction.
Improve Occlusal stability
Improved esthetics
Eliminate trauma from occlusion
Decreased occlusal stresses
Restorative longevity
More accurate treatment planning
Enhance functional occlusal
11.
FEATURES OF IDEALOCCLUSION
• The restored centric occlusion should coincide the centric relation -a repeatableposition.
• Cusp to fossa occlusion is preferred to enhance stability
• In centric occlusion, the supporting cusps of all posterior teeth occlude with marginal
ridges, except for the disto-buccal cusps of mandibular molars and the mesio-lingual
cusps of maxillary molars which occlude with central fossae of their opposing arch.
• No posterior interference and the anterior teeth disocclude posterior teeth protrusion
• Lateral working position maybe canine occlusion or group function.
12.
• Smooth andwhere possible uniform centric contacts
• Occlusal contacts should be in line with long axis of tooth
• Should allow for normal mastication, Deglutition,speech, esthetic and
respiratory functions.
• Healthy activity of the masticatory muscles
• No signs or symptoms of pain or dysfunction from any component of
masticatory system.
13.
Static Occlusion:
Classified intofour types:
Surface -to-Surface contact.
• It is also referring to as “mashed potato occlusion”.
• It is stressful, Produces lateral interferences in any function. Never used.
Tripod contact.
• In tripod contact the tip of the cusp never touches the opposing tooth.
✓ difficult to achieve.
✓ hard to adjust. limited in its use.
14.
Cusp-Ridge contact.
• It’salso called a “tooth-to-two-teeth” occlusion.
• “cusp-embrasure” occlusal pattern
Cusp tip-to-fossa contact.
• Also called “tooth-to-one-tooth”
• Cusp tip-to-fossa contact offers:
✓ excellent function.
✓ stability with flexibility.
✓ resistance to wear.
15.
Advantages of Cusp-Fossaover Cusp-Marginal Ridge Pattern of
occlusion:
• Produces an interlocking of the upper and lower teeth, thus giving
maximum support in centric occlusion.
• The forces are closer to the long axis of each tooth, giving a more
efficient chewing apparatus and less tipping.
• There is elimination of food impaction between marginal ridges.
• The teeth are more stable, with more stable occlusion, and lesser wear
of the cusp tips.
16.
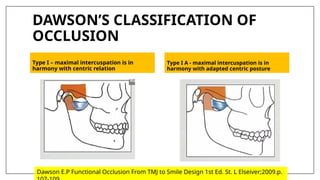
DAWSON’S CLASSIFICATION OF
OCCLUSION
TypeI – maximal intercuspation is in
harmony with centric relation
Type I A - maximal intercuspation is in
harmony with adapted centric posture
Dawson E.P Functional Occlusion From TMJ to Smile Design 1st Ed. St. L Elseiver;2009.p.
17.
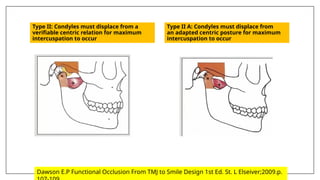
Type II: Condylesmust displace from a
verifiable centric relation for maximum
intercuspation to occur
Type II A: Condyles must displace from
an adapted centric posture for maximum
intercuspation to occur
Dawson E.P Functional Occlusion From TMJ to Smile Design 1st Ed. St. L Elseiver;2009.p.
18.
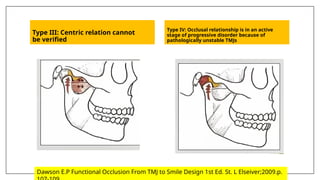
Type III: Centricrelation cannot
be verified
Type IV: Occlusal relationship is in an active
stage of progressive disorder because of
pathologically unstable TMJs
Dawson E.P Functional Occlusion From TMJ to Smile Design 1st Ed. St. L Elseiver;2009.p.
19.
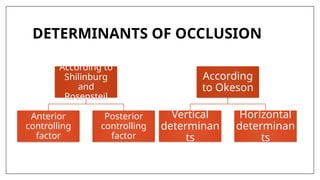
DETERMINANTS OF OCCLUSION
Accordingto
Shilinburg
and
Rosensteil
Anterior
controlling
factor
Posterior
controlling
factor
According
to Okeson
Vertical
determinan
ts
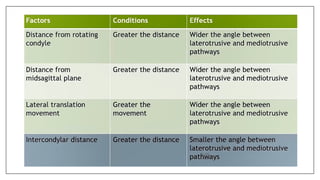
Horizontal
determinan
ts
20.
POSTERIOR CONTROLLING FACTOR
•The posterior determinants of mandibular movement are the
temporomandibular controls and their associated structures.
• These associated structures are:
1. Shape of the articular eminences
2. Anatomy of the medial walls of the mandibular fossae
3. Configuration of the mandibular condylar processes all of which
cannot be altered by the dentist
22.
ANTERIOR CONTROLLING FACTOR
•The anterior determinants are :
1. vertical overlap
2. horizontal overlap of the anterior teeth
3. the form of the lingual concavities of the maxillary anterior teeth
which can be altered by the operator.
• These determinants decide on the nature of the restoration or
rehabilitation work to be conducted,
for example: the height of the cusp can be determined
depending on how greater or lesser is the curve of Spee8.
24.
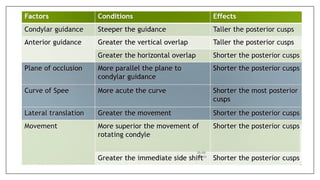
VERTICAL DETERMINANTS
• Factorsthat influence the height of the cusps and depth of the fossae
are the vertical determinants of occlusal morphology
• The length of a cusp and the distance it extends in to the depth of an
opposing fossa are determined by three factors:
1. Anterior guidance
2. Condylar guidance
3. Nearness of the cusp to these controlling factors
Bilateral balanced occlusion
•By von Spee and Monson.
• It dictates that a maximum number of
teeth should contact in all excursive
positions of the mandible.
• This is particularly useful in complete
denture construction, in which contact
on the nonworking side
• Is important to prevent tipping of the
denture.
• As trying this out in natural dentition
caused many wear faucets due to
excessive friction it was not advisable
to be used in natural dentition .
32.
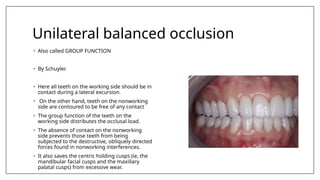
Unilateral balanced occlusion
•Also called GROUP FUNCTION
• By Schuyler.
• Here all teeth on the working side should be in
contact during a lateral excursion.
• On the other hand, teeth on the nonworking
side are contoured to be free of any contact
• The group function of the teeth on the
working side distributes the occlusal load.
• The absence of contact on the nonworking
side prevents those teeth from being
subjected to the destructive, obliquely directed
forces found in nonworking interferences.
• It also saves the centric holding cusps (ie, the
mandibular facial cusps and the maxillary
palatal cusps) from excessive wear.
33.
Long Centric:
• Longcentric or “Freedom in Centric” is an occlusal concept, in which a
flat region is built between the retruded position (CR) and the maximum
intercuspation (MIC), without a change in the vertical dimension.
• This flat region, having a length of 0.5-1mm, gives the mandible freedom
to close in Centric or slightly anterior to it without any interference.
• Cases that need Freedom in Centric:
1. When teeth are in the way if the patients close normally, but are fine
when the mandible is pushed to the back.
2. When teeth are fine when lying down, but are in the way while sitting
upright.
3. If a patient needs long centric and does not get it, bruxism and
clenching could happen.
34.
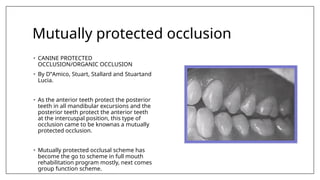
Mutually protected occlusion
•CANINE PROTECTED
OCCLUSION/ORGANIC OCCLUSION
• By D‟Amico, Stuart, Stallard and Stuartand
Lucia.
• As the anterior teeth protect the posterior
teeth in all mandibular excursions and the
posterior teeth protect the anterior teeth
at the intercuspal position, this type of
occlusion came to be knownas a mutually
protected occlusion.
• Mutually protected occlusal scheme has
become the go to scheme in full mouth
rehabilitation program mostly, next comes
group function scheme.
35.
In Maximum Intercuspation:
•All posterior teeth are in contact with the forces being directed along their long
axes.
• The anterior teeth either contact lightly or are very slightly out of contact (25
microns), relieving them of the obliquely directed forces that would be the result
of anterior teeth contact. As a result of the anterior teeth protecting the posterior
teeth in all mandibular excursions and the posterior teeth protecting the anterior
teeth at the intercuspal position.
When not to give mutually protected occlusion
1. presence of anterior bone loss
2. missing canines
3. class II or a class III malocclusion (angle classification), because the mandible
can not be guided by the anterior teeth.
4. Contraindicated in reverse occlusion, or cross bite, in which the maxillary and
mandibular buccal cusps interfere with each other in a working-side excursion
36.
OCCLUSAL INTERFERENCE
• anytooth contact that inhibits the remaining occluding surfaces
from achieving stable and harmonious contacts;
• any undesirable occlusal contact
37.
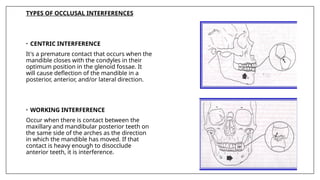
TYPES OF OCCLUSALINTERFERENCES
• CENTRIC INTERFERENCE
It's a premature contact that occurs when the
mandible closes with the condyles in their
optimum position in the glenoid fossae. It
will cause deflection of the mandible in a
posterior, anterior, and/or lateral direction.
• WORKING INTERFERENCE
Occur when there is contact between the
maxillary and mandibular posterior teeth on
the same side of the arches as the direction
in which the mandible has moved. If that
contact is heavy enough to disocclude
anterior teeth, it is interference.
38.
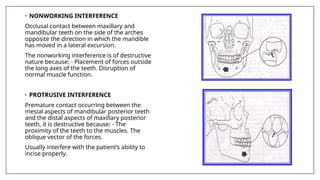
• NONWORKING INTERFERENCE
Occlusalcontact between maxillary and
mandibular teeth on the side of the arches
opposite the direction in which the mandible
has moved in a lateral excursion.
The nonworking interference is of destructive
nature because: - Placement of forces outside
the long axes of the teeth. Disruption of
normal muscle function.
• PROTRUSIVE INTERFERENCE
Premature contact occurring between the
mesial aspects of mandibular posterior teeth
and the distal aspects of maxillary posterior
teeth, it is destructive because: - The
proximity of the teeth to the muscles. The
oblique vector of the forces.
Usually interfere with the patient’s ability to
incise properly.
39.
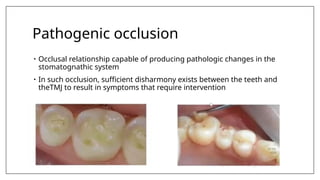
Pathogenic occlusion
• Occlusalrelationship capable of producing pathologic changes in the
stomatognathic system
• In such occlusion, sufficient disharmony exists between the teeth and
theTMJ to result in symptoms that require intervention
41.
OCCLUSAL TREATMENT
The objectiveof occlusal treatment are as follows:
1. To direct the occlusal forces along the long axes of the teeth
2. To attain simultaneous contact of all teeth in centric relation
3. To eliminate any occlusal contact on inclined planes to enhance the
positional stability of the teeth
4. To have centric relation coincide with the MIP
5. To arrive at the occlusal scheme selected for the patient
42.
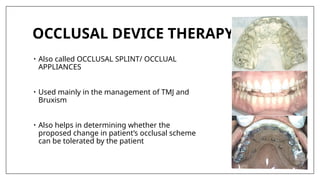
OCCLUSAL DEVICE THERAPY
•Also called OCCLUSAL SPLINT/ OCCLUAL
APPLIANCES
• Used mainly in the management of TMJ and
Bruxism
• Also helps in determining whether the
proposed change in patient’s occlusal scheme
can be tolerated by the patient
43.
Fabrication of occlusaldevice
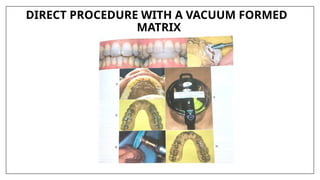
1. Direct procedure with a vacuum formed matrix
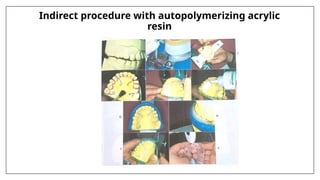
2. Indirect procedure with autopolymerizing acrylic resin
CONCLUSION
The controversy aboutocclusion cannot be resolved for three reasons:
1. Much knowledge is based upon empirical rather than scientific
information
2. If a certain concept failed in one specific mouth, it does not mean that
it would fail in all mouth.
3. The tremendous variable factor of the individual dentist and the
standards by which he evaluates his completed restoration.
47.
REFERENCES
• Dawson.P.E.Evaluation,Diagnosis andTreatment of occlusal
problems.St.Louis MO.CV Mobsy Co (1974)
• Okeson JP: Management of temperomandibular disorders and
occlusion 5 th edition st louis hyleermosby 2003;109- 126.
• Rosientiel:Contemporary fixed prosthesis fifth edition
• Shillingburg. Fundamentals of fixed prosthodontics: fourth edition



















![Prosthodontic management of endodontically treated teeth [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/prosthodonticmanagementofendodonticallytreatedteethautosaved-210611115147-thumbnail.jpg?width=640&height=640&fit=bounds)