Downloaded 141 times


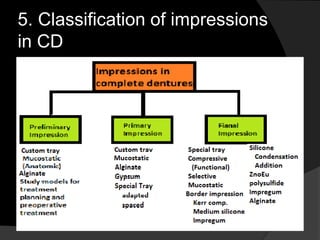
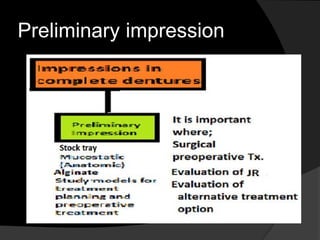
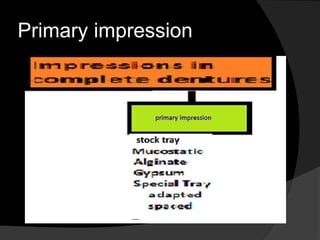
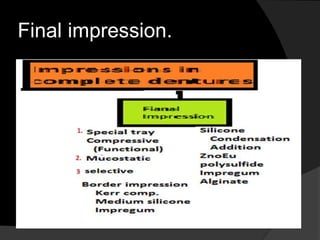





The document discusses the importance of making accurate impressions for conventional complete dentures, detailing the anatomical and physiological factors involved, and the significance of various impression materials and techniques. It covers patient examinations, classifications of impressions, and the roles of compressive, mucostatic, and selective pressure techniques in denture construction. The conclusion emphasizes the necessity of addressing issues like xerostomia and neurological disorders using denture adhesives to enhance retention and patient adaptation.