INTRODUCTION.
• Centric relation(CR) is a core topic of dentistry in general and
prosthodontics in particular.
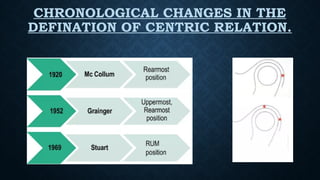
• The concept of CR emerged due to the search for a reproducible
mandibular position that would enable the prosthodontic rehabilitation.
• The term CR has become thoroughly confusing because of many
conflicting definitions. Unfortunately, definition of CR changed repeatedly
over past ten decades.
• Most of the controversies are pertaining to the position of the head of the
condyle in the glenoid fossa during centric relation position.
• This ranges from a retruded posterior position, to superior position and
then to an anterior superior position.
• A missed CR destroys the accuracy of even the most sophisticated
instrument system and can lead to failure of a prosthodontic treatment.
Palaskar JN, Murali R, Bansal S. Centric relation definition: a historical and contemporary prosthodontic perspective. J
Indian Prosthodont Soc. 2013 Sep;13(3):149-54. doi: 10.1007/s13191-012-0209-7. Epub 2012 Oct 31. PMID: 24431728;
PMCID: PMC3732724.
4.
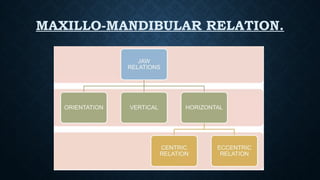
DEFINITION.
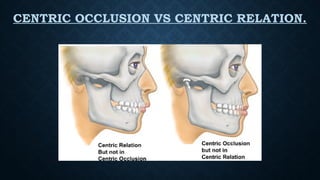
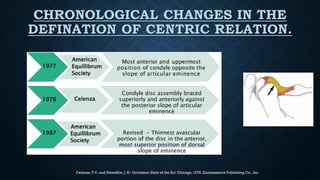
• CENTRIC RELATION:A maxillomandibular relationship, independent of tooth contact, in
which condyles articulate in the anterior-superior position against the posterior slopes of
articular eminence in this position, the mandible is restricted to a purely rotary movement;
from this un strained, physiologic, maxillomandibular relationship, the patient can make
vertical, lateral or protrusive movements; it is a clinically useful, repeatable reference position.
GPT-9
• CENTRIC OCCLUSION: ‘The Complete Intercuspation of the opposing teeth independent of
condylar position’. GPT 9.
• CENTRIC RELATION RECORD: A Registration of relationship of Maxilla to Mandible when
Mandible is in Centric Relation. May be obtained Intraorally or Extra orally.
• TERMINAL HINGE AXIS/TRANSVERSE HORIZONTAL AXIS: An imaginary line around which
the mandible may rotate within the sagittal plane.
• NOTE: The rearmost position is relative term which denotes that the condyles can go backwards as
far as the temporomandibular ligaments would permit without any strain.
• It does not literally mean the most retruded position in the glenoid fossa, since such a position will
produce considerable amount of strain in ligaments and cause pain.
Celenza, F.V., andNasedkin, J. N.: Occlusion: State of the Art. Chicago, 1978, Quintessence Publishing Co., Inc.
8.
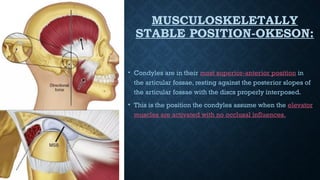
MUSCULOSKELETALLY
STABLE POSITION-OKESON:
• Condylesare in their most superior-anterior position in
the articular fossae, resting against the posterior slopes of
the articular fossae with the discs properly interposed.
• This is the position the condyles assume when the elevator
muscles are activated with no occlusal influences.
9.
SIGNIFICANCE OF CENTRICRELATION.
• Bone to bone relation (constant).
• Repeatable and recordable and thus
serves as a reliable guide for
developing centric occlusion.
• Related to the terminal hinge axis, in
centric relation, condyles exhibit pure
rotation without any translation.
• More definite than vertical relation
since it is independent of tooth contact.
Yurkstas AA, Kapur KK. Factors influencing centric relation records in edentulous mouths. J Prosthet Dent 2005- 93 305-10
10.
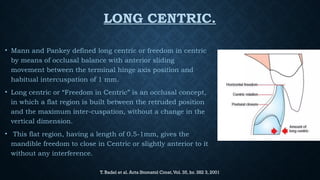
LONG CENTRIC.
• Mannand Pankey defined long centric or freedom in centric
by means of occlusal balance with anterior sliding
movement between the terminal hinge axis position and
habitual intercuspation of 1 mm.
• Long centric or “Freedom in Centric” is an occlusal concept,
in which a flat region is built between the retruded position
and the maximum inter-cuspation, without a change in the
vertical dimension.
• This flat region, having a length of 0.5-1mm, gives the
mandible freedom to close in Centric or slightly anterior to it
without any interference.
T. Badel et al. Acta Stomatol Croat,Vol. 35, br. 382 3, 2001
11.
FACTORS THAT DETERMINECENTRIC
RELATION.
Resiliency of the supporting tissues.
Stability of the recording bases.
Temporomandibular joint and its associated neuromuscular mechanisms .
Character of the pressure applied in making the records .
Technique used in making the records and the associated recording devices used.
Skill of the dentist.
Health and cooperation of the patient.
Maxillomandibular relationship.
Posture of the patient.
Character or size of the residual alveolar arch.
Amount and character of the saliva.
Size and position of the tongue.
Yurkstsas and kapur. Centric relation records in edentulous mouths. J.
Pros. Den. Nov 1964
12.
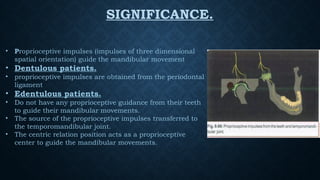
SIGNIFICANCE.
• Proprioceptive impulses(impulses of three dimensional
spatial orientation) guide the mandibular movement
• Dentulous patients.
• proprioceptive impulses are obtained from the periodontal
ligament
• Edentulous patients.
• Do not have any proprioceptive guidance from their teeth
to guide their mandibular movements.
• The source of the proprioceptive impulses transferred to
the temporomandibular joint.
• The centric relation position acts as a proprioceptive
center to guide the mandibular movements.
13.
SIGNIFICANCE.
Serves asa reliable guide to develop centric occlusion in complete dentures.
Centric relation become starting point to plan and execute the occlusion.
Centric relation is related to terminal hinge axis.
In centric relation, condyles exhibit pure rotation without any translation.
14.
SALIENT FEATURES.
• Learnable,repeatable and recordable position,
• Remains constant throughout life.
• Purely rotary movements occur.
• Unstrained, physiologic relationship.
• Mandible can move to any eccentric position and return back involuntarily. It acts as a center
from which all movements can be made.
• If the mandible has to move from one eccentric position to another it should go to centric
relation before advancing to the target eccentric position.
• Functional movements like chewing and swallowing are performed in this position, because it is
the most unstrained position.
15.
• The musclesthat act on TMJ are arranged in such a way that it is easy to move the
mandible to centric position from where all the movements can made.
• The casts should be mounted in centric relation because it is the point from which all
the movements can be made or simulated in the articulator.
• It is helpful in adjusting condylar guidance in an articulator to produce balanced
occlusion.
• It is a definite entity, so it is used as reference point in establishing centric occlusion.
16.
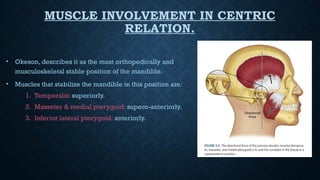
MUSCLE INVOLVEMENT INCENTRIC
RELATION.
• Okeson, describes it as the most orthopedically and
musculoskeletal stable position of the mandible.
• Muscles that stabilize the mandible in this position are:
1. Temporalis: superiorly.
2. Masseter & medial pterygoid: supero-anteriorly.
3. Inferior lateral pterygoid: anteriorly.
17.
DIFFICULTIES IN RETRUDINGMANDIBLE
CAN BE CLASSIFIED AS :
Biological causes-
a. Lack of muscle coordination in opposing groups.
b. Patient closing habitually in protruded relation.
Psychological causes-
a. Patient unable to follow instructions due to anxiety and stress.
Mechanical causes-
a. Poor adaptation of record bases.
18.
RECORDING MATERIALS.
Waxes:Hard baseplate or reinforced (Aluwax, Coprawax):. The material is generally considered
too unstable and inaccurate for CR but can be used successfully for static (positional) lateral
checkbites.
Compound (modeling plastic): accurate but are technique sensitive. Need to have uniform
softening to prevent uneven pressure while recording CR.
Plaster and ZOE: accurate and stable but difficult and messy to use.
Elastomeric are stable, easy to use and acceptable accuracy.
A) PHYSIOLOGICAL METHOD.
•Physiological methods are called so because they are based on:
• -The proprioceptive impulses of the patient.
• - Kinesthetic sense of mandibular movement.
• - The visual acuity and sense of touch of the dentist.
• - No pressure is exerted on the interocclusal record.
• 2) PRESSUREMETHOD:
After establishing vertical dimension, the upper occlusal rim is placed in the
patient’s mouth.
The lower occlusal rim is fabricated to be of excess height.
Entire lower rim is softened in a water bath and inserted in the patient’s mouth.
Patient is guided to close his mouth in centric relation.
The patient is asked to close on the soft wax.
After the patient closes his mouth till the predetermined vertical dimension, both
rims are removed, cooled and articulated.
26.
B) FUNCTIONAL ORCHEW IN METHOD:
Functional movements of jaws are utilized.
Patient asked to perform border movements (Protrusive and lateral excursive movements) in
order to identify the most retruded position of the mandible.
• Advantage-
• vertical dimension and centric relation can be determined.
• Disadvantages-
• Inaccuracy due to - i)displaceable basal seat tissue,
ii) resistance of recording medium,
iii) due to lack of equalized pressure.
• Patient must have good neuromuscular co-ordination and be capable of following instructions.
27.
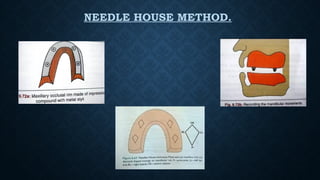
1) NEEDLE HOUSEMETHOD.
• Most commonly used functional technique.
• Occlusion rims are fabricated.
• Four metal beads or styli embedded in the premolar and molar areas of maxillary occlusion rims
• Occlusion rims inserted into the patient’s mouth.
• Patient asked to close on occlusion rims and make protrusive, retrusive , right and left lateral
movements of the mandible.
• On moving the mandible , the metal styli on the maxillary occlusion rim will create a marking on
the mandibular occlusion rim.
• A diamond shaped marking pattern is formed on the mandibular occlusion rim.
3) MEYER’S METHOD.
•Meyer used soft wax to generate the functional pathway and record centric
relation.
• Soft wax occlusal rims.
• Tinfoil was placed over wax and lubricated.
• Pt performs functional movements to produce a wax path.
• Plaster index was made.
Centric jaw relation –a critical evaluation of various methods –Sanjay bansal
Centric relation records-Historical review Michael L. Myers, D.M.D. * Medical University of South Carolina, College of Dental
Medicine, Charleston, S.C
FACTORS TO BECONSIDERED WHILE
CARRYING OUT TRACING:
Stability of denture base.
Resistance of rims.
Difficulty in placing central bearing device.
Height of residual alveolar ridge.
Tongue interference.
Efficiency of recording device.
Lack of coordinated movements.
33.
GOTHIC ARCH TRACING.
GOTHIC ARCH TRACER- the device, that produces a tracing
that resembles an arrowhead or a gothic; the device is
attached to the opposing arches, the shape of the tracing
depends on the relative location of the marking point and the
tracing table; the apex of a properly made tracing is
considered to indicate centric relation (GPT 4)
Synonyms- Arrow head tracing,Central bearing tracing,Needle
point tracing,Stylus tracing.
Gothic arch tracing was first proposed by- Hesse in 1897.
Later popularised by - Alfred Gysi in 1910 with a device called
as Gysi’s Recording Device.
34.
• ADVANTAGES:
Mostaccurate method of verifying Centric relation.
Allows equalization of pressure on supporting tissues.
Eccentric relations are also recorded for programming of semi-adjustable
articulator.
• DISADVANTAGES:
Time consuming.
Very cumbersome for the patient.
Training the patient in making mandibular movements is strenuous.
35.
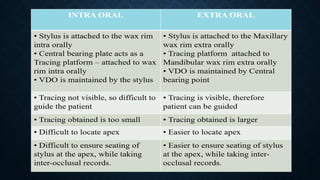
TYPES OF GOTHICARCH TRACING.
INTRA ORAL.
Central bearing point
and Tracing device are
located Intraorally.
EXTRA ORAL.
Central bearing device
located intraorally and
Tracing unit located
Extra orally.
36.
PARTS OF GOTHICARCH TRACER.
A. Intraoral Gothic Arch Tracers
1. Central bearing plate / Tracing plate
2. Central bearing point with stylus
B. Extraoral Gothic Arch Tracers
1. Central bearing device
Central bearing plate
Central bearing point
2. Tracing device
Stylus/Scriber point
Tracing plate/platform
37.
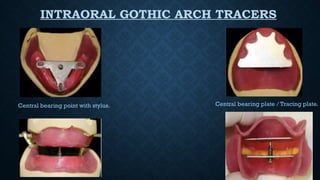
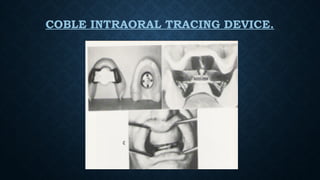
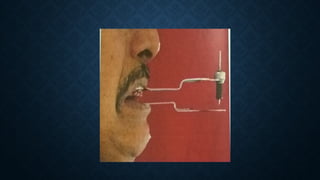
INTRAORAL GOTHIC ARCHTRACERS
Central bearing point with stylus. Central bearing plate / Tracing plate.
38.
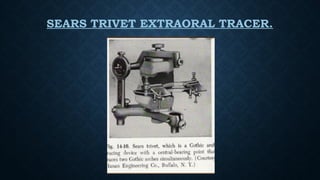
EXTRAORAL GOTHIC ARCHTRACERS.
CENTRAL BEARING PLATE. CENTRAL BEARING POINT.
STYLUS/SCRIBER POINT. TRACING PLATE/PLATFORM.
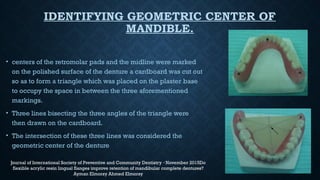
IDENTIFYING GEOMETRIC CENTEROF
MANDIBLE.
• centers of the retromolar pads and the midline were marked
on the polished surface of the denture a cardboard was cut out
so as to form a triangle which was placed on the plaster base
to occupy the space in between the three aforementioned
markings.
• Three lines bisecting the three angles of the triangle were
then drawn on the cardboard.
• The intersection of these three lines was considered the
geometric center of the denture
Journal of International Society of Preventive and Community Dentistry November 2015Do
·
flexible acrylic resin lingual flanges improve retention of mandibular complete dentures?
Ayman Elmorsy Ahmed Elmorsy
45.
ATTACHMENT OF TRACERS.
•Fixing the central bearing plates:
• Reduce the mandibular occlusion rim height by 4mm and make sure to have parallel walled
space between the occlusion rims
• Fix the central bearing point ,the surface of rim and the plate should be same
• Fix the maxillary central bearing plate
• The central bearing plate – resin base junction should be reinforced with sticky wax to prevent
sinking of the central bearing plates during tracing
An insight into gothic arch tracing S.U. Meghana Gajavalli
47.
ATTACHMENT OF TRACERS.
•Fixing the extra oral tracer:
• Lower member of the Hight tracer is fixed to the mandibular occlusion rim 3mm below the
modified occlusal plane and maintain parallelism
• The upper member of the tracer is fixed to maxillary occlusion rim 3mm above the occlusion
plane parallel to lower member of tracing unit with sticky wax
• The stylus should just touch the tracing table.
48.
ATTACHMENT OF TRACERS.
•Tracing :
• Place both the bases in the mouth and smear the surface of the maxillary plate with petroleum jelly.
• Coat the tracing table with a mix of zinc oxide and spirit with a flat brush no.5 .
• Apply with single strokes and allow it to dry and ask the patient to close the mouth in centric.
• Repeat three times-ask the patient to protrude and go back without any restriction.
49.
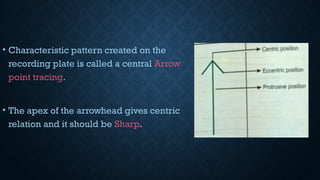
• Characteristic patterncreated on the
recording plate is called a central Arrow
point tracing.
• The apex of the arrowhead gives centric
relation and it should be Sharp.
54.
INTRAORAL TRACINGS.
Centralbearing device is located intraorally.
Advantages:
Capturing VDO and CR in an easy-to-use technique for practitioners.
Intraoral tracing (Gothic arch tracing) is a preferred method of obtaining consistent
positions of the mandible in motion (retrusive, protrusive and lateral) at a comfortable
VDO.
• Disadvantages:
• Tracer is not visible during this procedure.
• Area size of the tracing is very small, hence difficult to determine the tracing.
55.
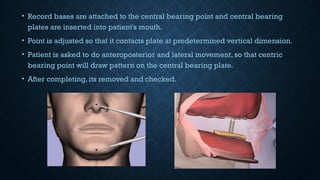
• Record basesare attached to the central bearing point and central bearing
plates are inserted into patient's mouth.
• Point is adjusted so that it contacts plate at predetermined vertical dimension.
• Patient is asked to do anteroposterior and lateral movement, so that centric
bearing point will draw pattern on the central bearing plate.
• After completing, its removed and checked.
57.
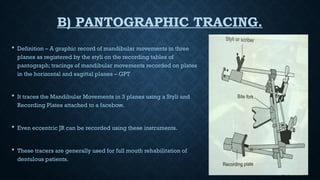
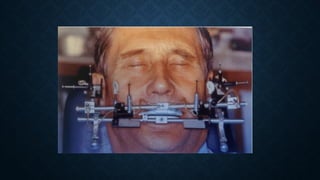
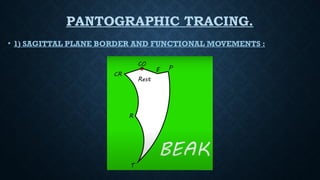
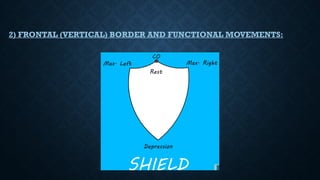
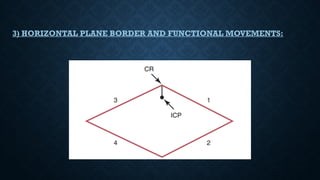
B) PANTOGRAPHIC TRACING.
Definition – A graphic record of mandibular movements in three
planes as registered by the styli on the recording tables of
pantograph; tracings of mandibular movements recorded on plates
in the horizontal and sagittal planes – GPT
It traces the Mandibular Movements in 3 planes using a Styli and
Recording Plates attached to a facebow.
Even eccentric JR can be recorded using these instruments.
These tracers are generally used for full mouth rehabilitation of
dentulous patients.
58.
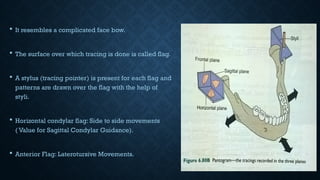
It resemblesa complicated face bow.
The surface over which tracing is done is called flag.
A stylus (tracing pointer) is present for each flag and
patterns are drawn over the flag with the help of
styli.
Horizontal condylar flag: Side to side movements
( Value for Sagittal Condylar Guidance).
Anterior Flag: Laterotursive Movements.
RETRUDING THE MANDIBLE.
To record CR, mandible must be
retruded.
Various methods used to retrude
mandible are:-
1. Guided Method - by dentist.
2. Unguided Method - by patient.
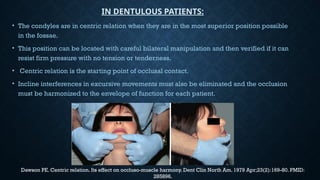
64.
• The condylesare in centric relation when they are in the most superior position possible
in the fossae.
• This position can be located with careful bilateral manipulation and then verified if it can
resist firm pressure with no tension or tenderness.
• Centric relation is the starting point of occlusal contact.
• Incline interferences in excursive movements must also be eliminated and the occlusion
must be harmonized to the envelope of function for each patient.
Dawson PE. Centric relation. Its effect on occluso-muscle harmony. Dent Clin North Am. 1979 Apr;23(2):169-80. PMID:
285896.
IN DENTULOUS PATIENTS:
• Dawson introducedbimanual mandibular manipulation to guide the
mandible to CR, defined as the most superior position of the condyle in
the glenoid fossa.
• Many researchers who support the most posterior position of the
condyle as CR to achieve proper positioning using chin point guidance
or Gothic arch tracing.
67.
ECCENTRIC JAW RELATION.
Definition–
Any relation of the mandible to the maxilla other than centric relation (GPT 9)
It includes protrusive and lateral relations .
Done to adjust the horizontal and lateral condylar inclination in the articulator.
Balanced occlusion can be established .
Can be recorded using functional or tactile methods .
It includes:
1)Protrusive relation.
2) Lateral relation.
Left lateral.
Right lateral.
68.
CEPHALOMETRICS.
The useof cephalometric to record centric relation was described by Pyott
and Schaeffer.
The proper centric relation and vertical dimension of occlusion were
determined by cephalometric radiographs.This method, however, was
somewhat impractical and never gained widespread usage.
69.
BOOSTS probablycame closest to the solution when he stated that “in
normal cases, the occlusion, the temporomandibular joints, the bone, the
soft tissue, and the musculature all produce the same relation to each
other and any one of the many registration techniques may be used.”
A certain technique might be required for an unusual situation or a
problem patient. In the final analysis, the skill of the dentist and the
cooperation of the patient are probably the most important factors in
securing an accurate centric relation record.
70.
CONSEQUENCES OF INCORRECT
CENTRICRELATION.
• 1.TMJ dysfunction : Condyle press upon peripheral vascular and
Innervated parts of Articular Disc.
• 2. Mucosal ulceration and irritation.
• 3. Pain and Dysfunction of Masticatory Muscles, Headache, Neck and
Shoulder Pain.
• 4. Resorption of Residual Alveolar Ridges.
• 5. Natural Dentition: Damage to periodontal structures, Hypersensitivity,
Excessive Attrition and Hypermobility of teeth.
71.
CONCLUSION.
The accuratedetermination, recording and transfer of jaw relation
records from edentulous patient to articulator is essential for restoring
function, facial appearance and maintenance of patients health.
Unsatisfactory maxillomandibular relations will eventually lead to
failure of complete denture.
72.
REFERENCES.
• Palaskar JN,Murali R, Bansal S. Centric relation definition: a historical and contemporary prosthodontic
perspective. J Indian Prosthodont Soc. 2013 Sep
• Ramaswamy, Kore-Techniques to Guide the Mandible to Centric Relation- A Systematic Review-DOI:
10.7860/JCDR/2021/49799.15083
• Dawson PE. Centric relation. Its effect on occluso-muscle harmony. Dent Clin North Am. 1979
Apr;23(2):169-80. PMID: 285896.
• Syllabus of complete denture: Heartwell 4th
edition
• Kantor, Silverman, and Garfinkel. Centric-relation recording techniques-a comparative investigation J.
l’rosthet. Dent. December, 1972
• Michael L. Myers, Centric relation records. The journal of prosthej’jc dentistry february 1982 volume 47
number 2
• Yurkstsas and kapur. Centric relation records in edentulous mouths. J. Pros. Den. Nov 1964
• Bhagat, et al.: Indigenous digital intra-oral gothic arch tracer. The Journal of Indian Prosthodontic Society
.Volume 19; Issue 2, April-June 2019