Downloaded 842 times


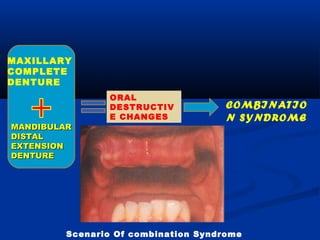
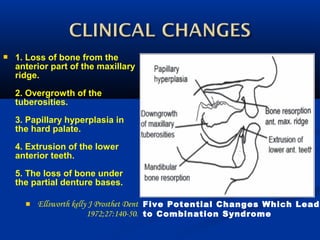
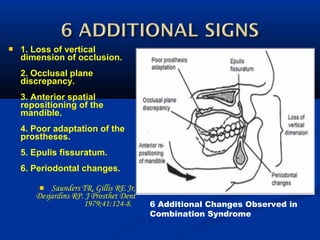
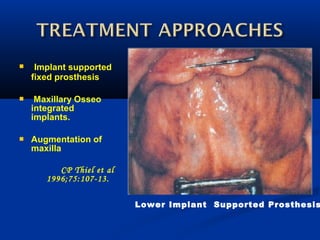
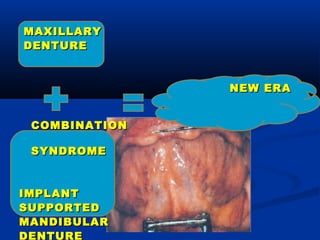


This document discusses combination syndrome, which occurs when a complete maxillary denture is opposed by a mandibular removable partial denture. This can lead to bone loss in the maxilla, enlargement of the mandibular tuberosities, and poor denture stability. Implant-supported prostheses and paying careful attention to occlusion design and retention are recommended to prevent these issues.














































