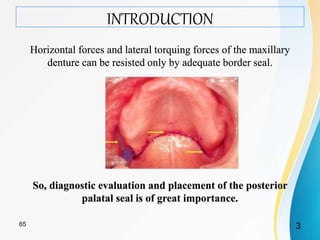
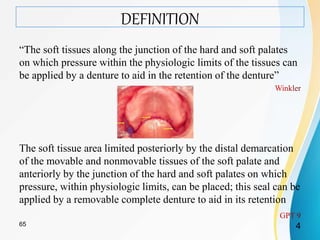
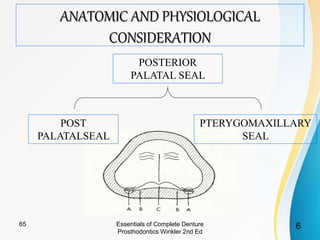
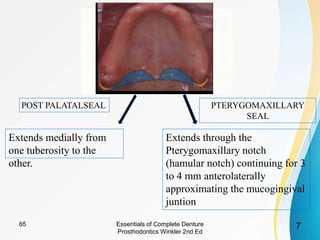
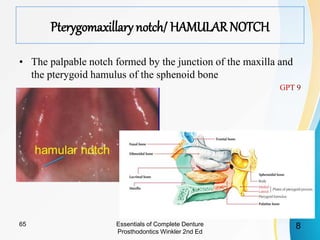
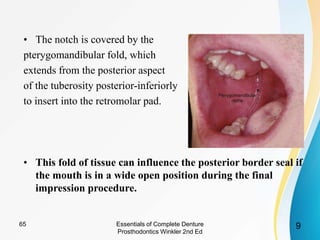
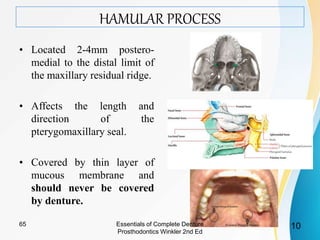
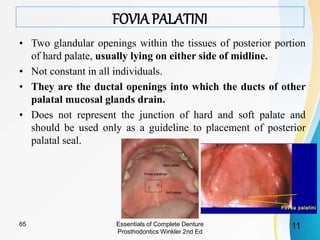
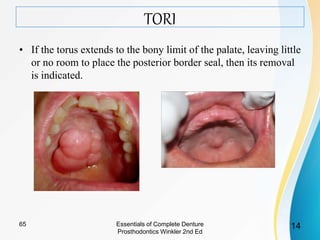
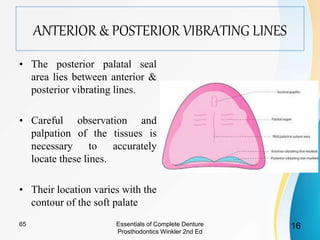
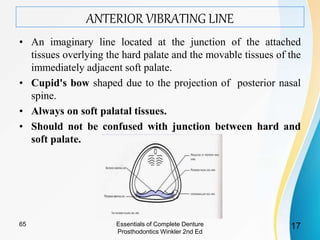
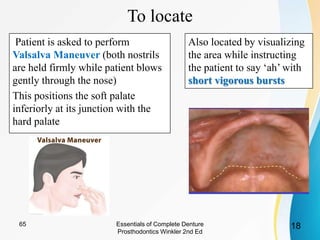
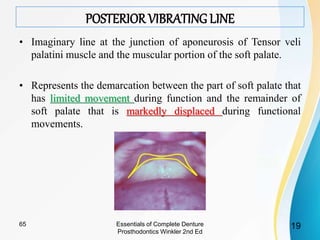
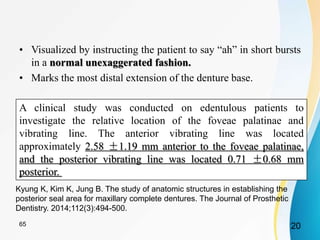
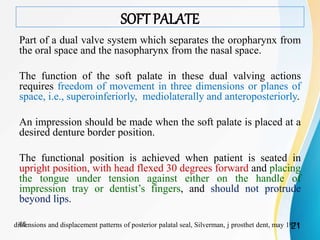
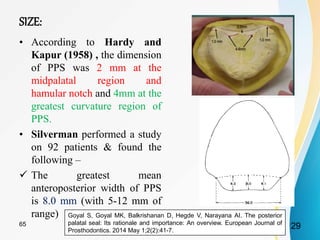
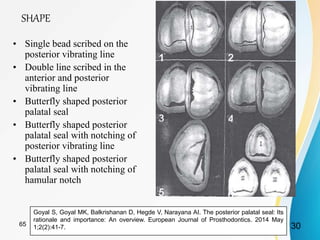
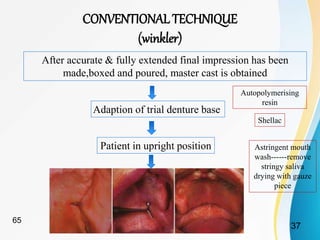
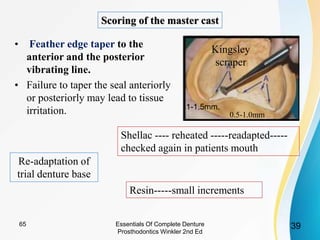
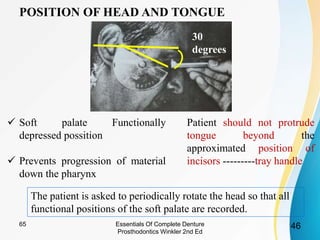
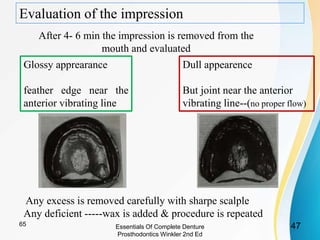
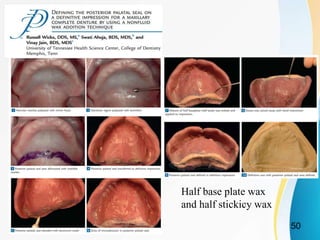
This document discusses the posterior palatal seal, which is the area of soft tissue along the junction of the hard and soft palates that can be compressed by a maxillary denture to aid in retention. It defines the posterior palatal seal and describes its functions, which include resisting forces on the denture and maintaining contact during function. The document outlines important anatomical structures like the vibrating lines and hamular notch that influence determination of the posterior palatal seal area. It also discusses techniques for locating and marking the seal, as well as factors that must be considered like a patient's soft palate classification.