The document discusses the principles of occlusion, including:
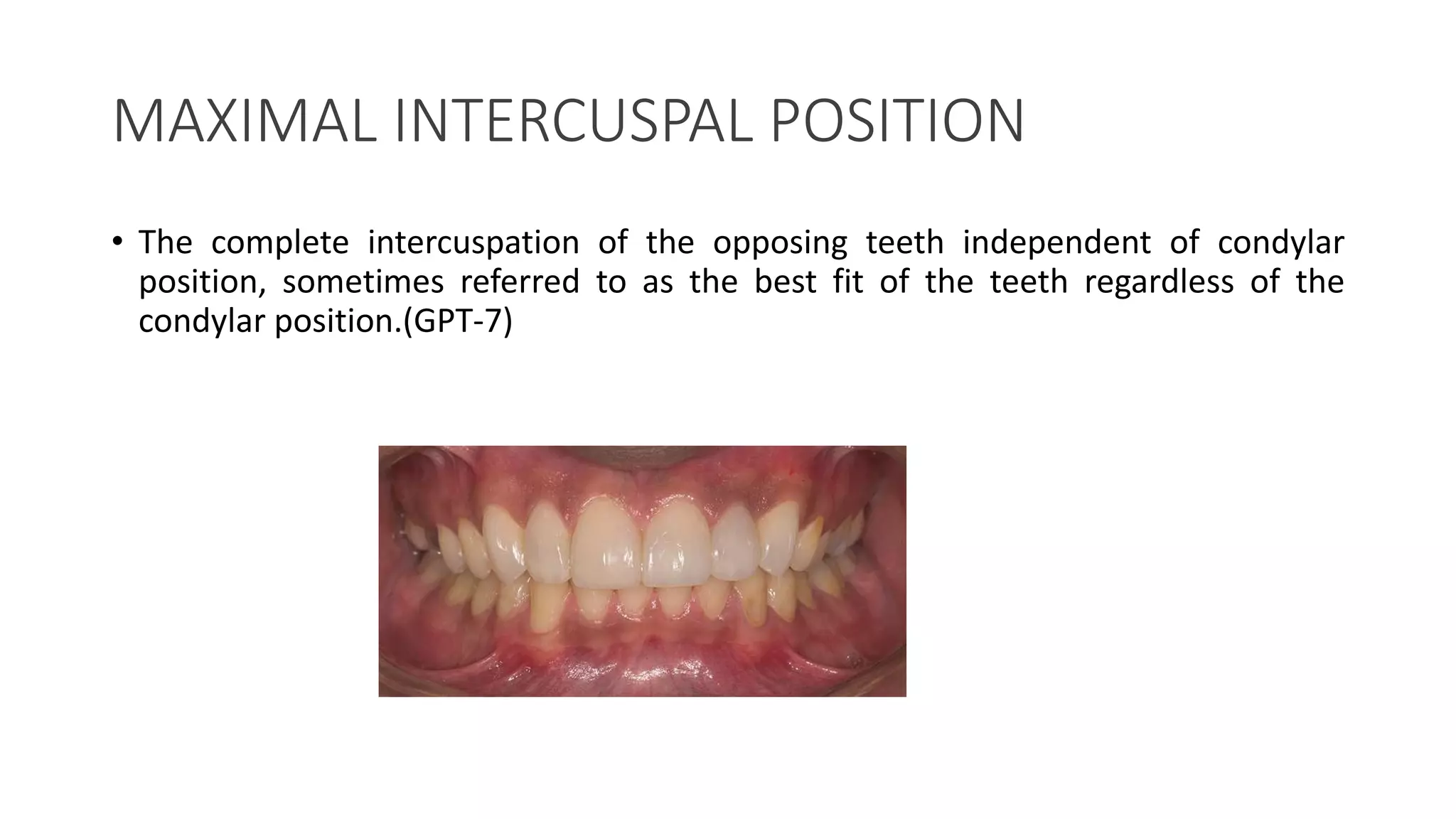
1) Maximal intercuspation should occur around centric relation for optimal occlusal stability and function.
2) Occlusion should provide mutually protected contact of teeth to avoid damage during jaw movements.
3) Proper anterior guidance is key to allow jaw function without interference.
4) Non-working side teeth should not contact during lateral excursions.
5) Posterior teeth occlusion should be reconstructed to mimic neighboring teeth.
Following these principles leads to long-term restoration success, while deviations can cause tooth and restoration damage over time.


















































![occlusion mmmmmmmm- Copy [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/occlusion-copyautosaved-240715160312-7fd34768-thumbnail.jpg?width=640&height=640&fit=bounds)