This document provides an overview of occlusion evaluation and therapy. It defines key terminology related to occlusion and mandibular movements. It describes the components of the masticatory system and discusses normal occlusion and occlusal dysfunction. The document outlines clinical evaluation procedures for occlusion including TMD screening, tooth mobility testing, and cast analysis. It discusses occlusal appliance therapy and requirements for occlusal stability. The summary emphasizes evaluation of occlusion, use of appliances to encourage tooth tightening, and progressive occlusal adjustment.


![BORDER
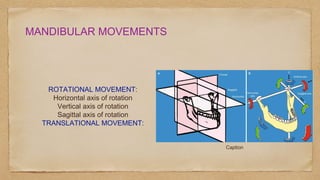
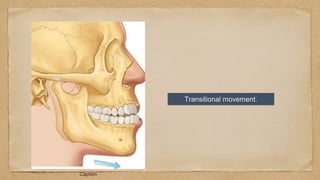
MOVEMENTS
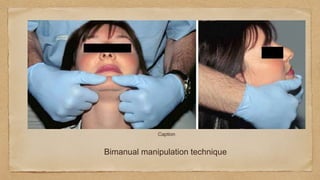
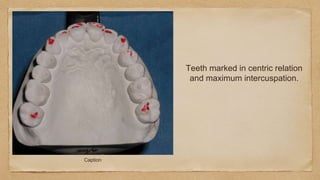
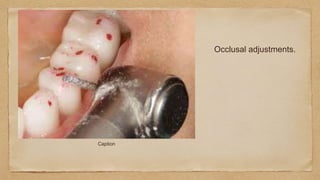
Caption
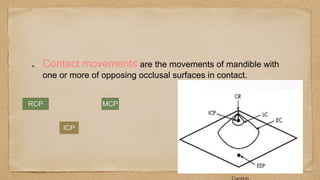
POSSELT ,1952
PR=PROTRUSION
ICP=INTERCUSPAL
POSITION
RCP=RETRUDED
CONTACT POSITION
R[HA]=HINGE AXIS
T[MO]=MAXIMUM OPENING](https://image.slidesharecdn.com/bhavyaocclusalevaluation-231007101551-e19b648b/85/Occlusal-evaluation-pptx-16-320.jpg)






































![occlusion mmmmmmmm- Copy [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/occlusion-copyautosaved-240715160312-7fd34768-thumbnail.jpg?width=640&height=640&fit=bounds)





















































