Downloaded 48 times
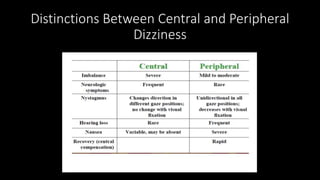
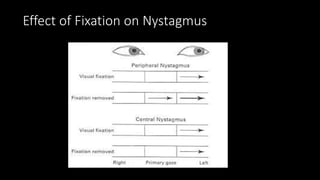
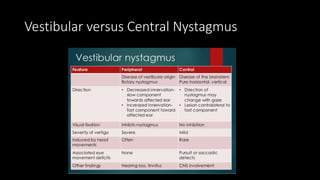
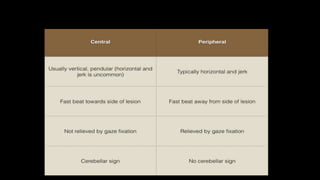
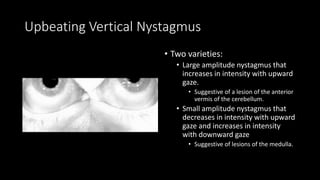
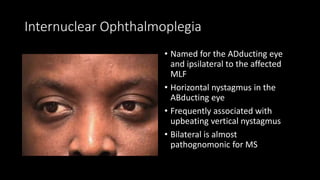

This document discusses various types of central nystagmus and vertigo, including their distinguishing characteristics and potential causes. Central positional vertigo can be caused by lesions in the cerebellum. Direction changing nystagmus suggests a problem holding gaze due to cerebellar or brainstem issues. Upbeating or downbeating vertical nystagmus localize to specific areas of the cerebellum or brainstem. Internuclear ophthalmoplegia is associated with multiple sclerosis. Rebound nystagmus indicates brainstem or cerebellar disease.

































































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)


