Download to read offline
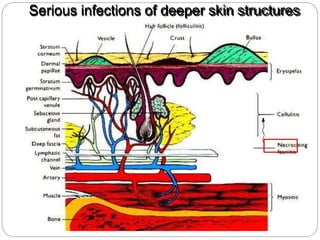
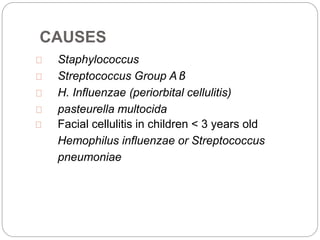








Cellulitis is an acute infection of the deeper layers of skin and subcutaneous tissue, often caused by Staphylococcus or Streptococcus bacteria. It presents with red, warm, painful, and swollen skin that may have pus and fever. Risk factors include local skin injuries or infections. Treatment involves antibiotics, elevation, and warm compresses to resolve the infection and prevent spread. More severe cases may rapidly progress to necrotizing fasciitis so aggressive treatment is needed.













































![Cellulites [ compatibility mode].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cellulitescompatibilitymode-221125052621-3abc2023-thumbnail.jpg?width=640&height=640&fit=bounds)









































