Downloaded 12 times














![INITIAL RESUSCITATION [1st 6 hrs]
• Central venous pressure (CVP): 8–12 mm
Hg / 12-15 if mechanical ventilation
• Mean arterial pressure (MAP) >65 mm Hg
• Urine output >0.5 mL/kg/hour
• Central venous (superior vena cava) or
mixed venous oxygen saturation >70% or
>65%, respectively](https://image.slidesharecdn.com/sepsis-190613051634/85/Sepsis-17-320.jpg)




























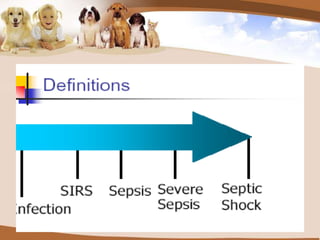
This document discusses sepsis, a systemic inflammatory response to infection that can lead to organ dysfunction. It defines terms like systemic inflammatory response syndrome (SIRS), sepsis, severe sepsis, and septic shock. The pathogenesis involves inflammation, coagulation, and cytokines. Management involves initial resuscitation, diagnosis via blood cultures, antibiotics, source control, hemodynamic support with vasopressors and inotropes, steroids, mechanical ventilation, glucose control, renal replacement if needed, and DVT prophylaxis. Outcomes have improved with early goal directed therapy, lung protective ventilation, appropriate antibiotics, activated protein C, tight glucose control, and steroids.























































































