Downloaded 148 times

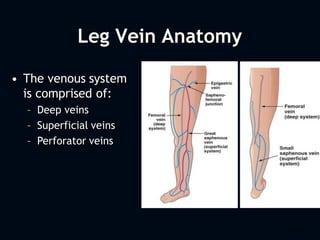
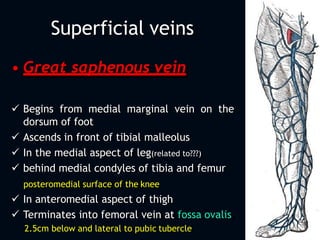
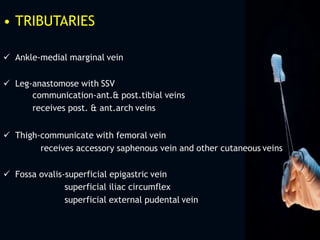
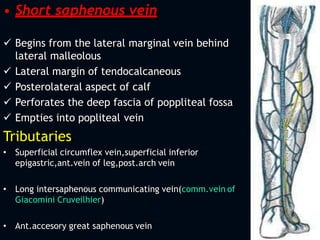
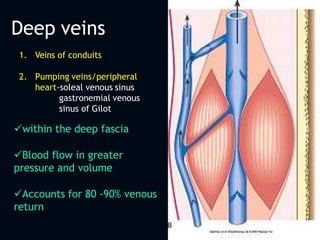
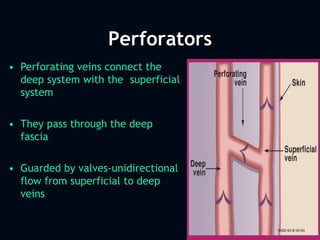
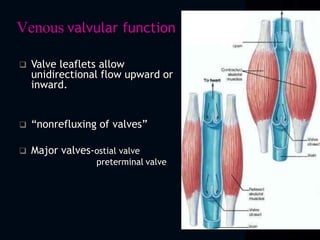
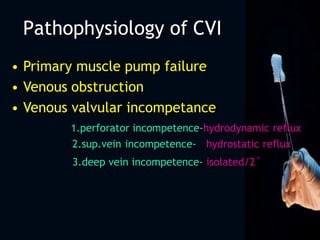
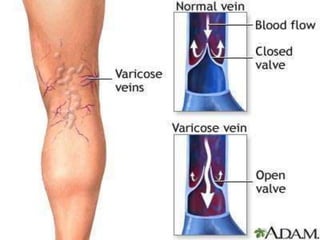
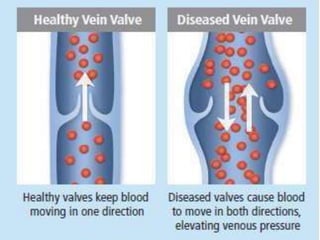
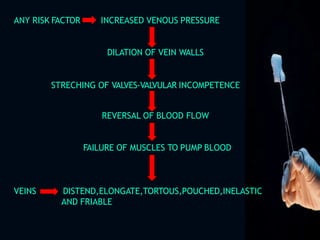
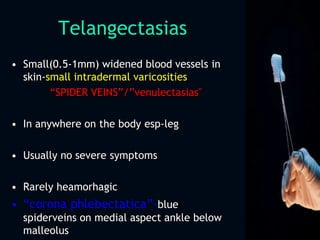

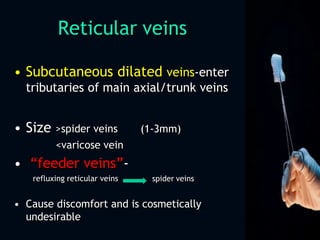


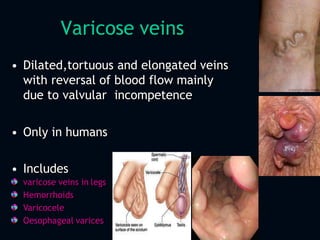


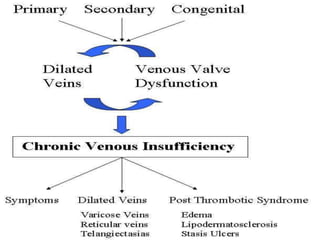






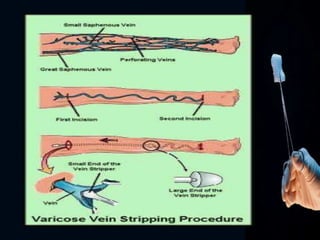
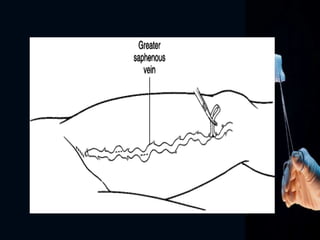
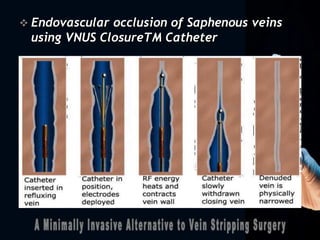

This document summarizes chronic venous insufficiency (CVI), which occurs when veins cannot pump enough deoxygenated blood back to the heart. CVI mainly affects the legs and can cause varicose veins, spider veins, and reticular veins. The venous system includes deep, superficial, and perforating veins. The great and short saphenous veins are major superficial leg veins. CVI is caused by primary muscle pump failure, venous obstruction, or valvular incompetence. It can lead to complications like ulcers, pigmentation changes, and lipodermatosclerosis. Treatment includes conservative measures, sclerotherapy, and surgical procedures like vein stripping to remove damaged veins.






















































































