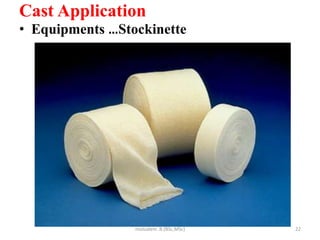
The document discusses casts, including their definition, types, application process, and removal process. It defines a cast as a rigid external device used to immobilize and support fractures, deformities, and injuries. It describes various types of casts such as short arm, long arm, short leg, and shoulder spica casts. It provides a 12 step process for applying a plaster cast including prepping the patient and area, applying stockinette, cotton, and plaster, and molding and drying the cast. It also outlines the equipment and steps for cast removal using a saw and spreaders.




















































































































































![Care of bedridden patient [cast]](https://cdn.slidesharecdn.com/ss_thumbnails/careofbedriddenpatientcast-210720163147-thumbnail.jpg?width=640&height=640&fit=bounds)












































