
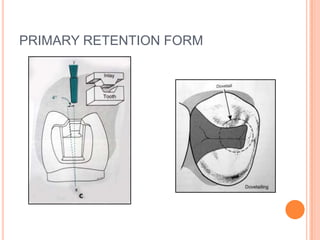
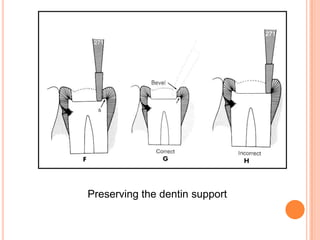
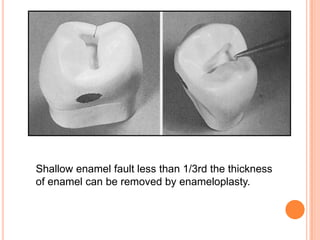
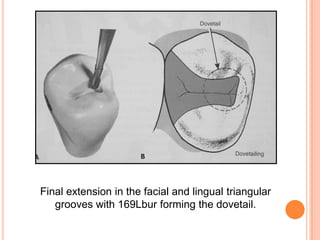
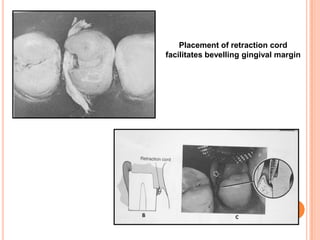
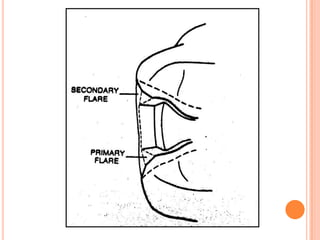
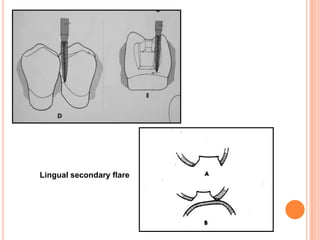
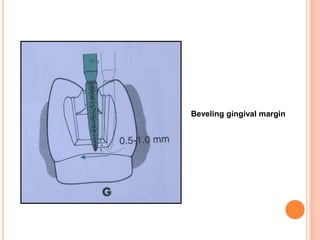
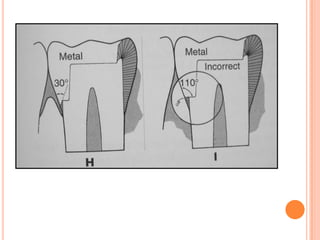
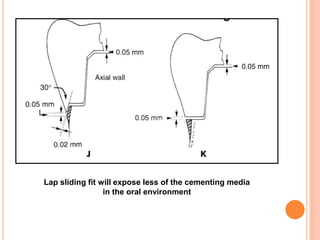
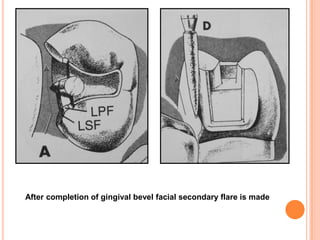
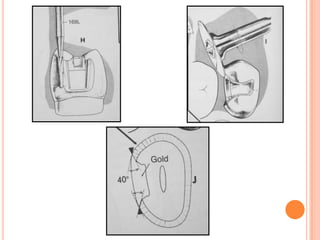
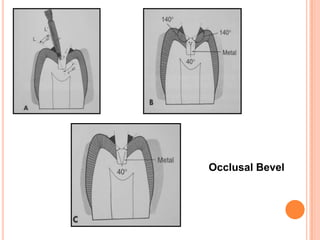
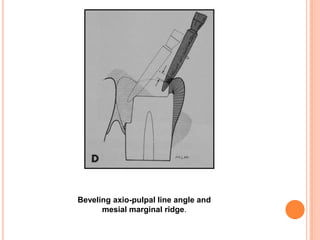
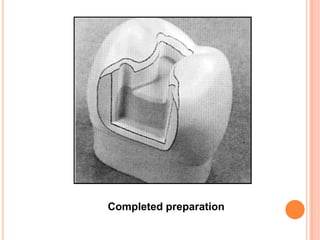



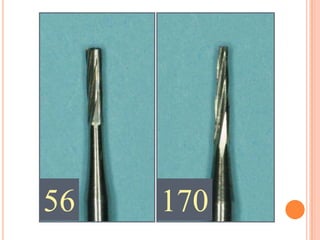
















The document discusses the principles and techniques for cast metal inlay restorations, including materials used, indications and contraindications, advantages and disadvantages. It covers cavity design considerations like apico-occlusal taper, convergence angles, and preparation features. Furthermore, it examines bevel designs and their significance in strengthening tooth structure and improving marginal adaptation of cast restorations.














































































